Aetnamedicare.com Phi Form
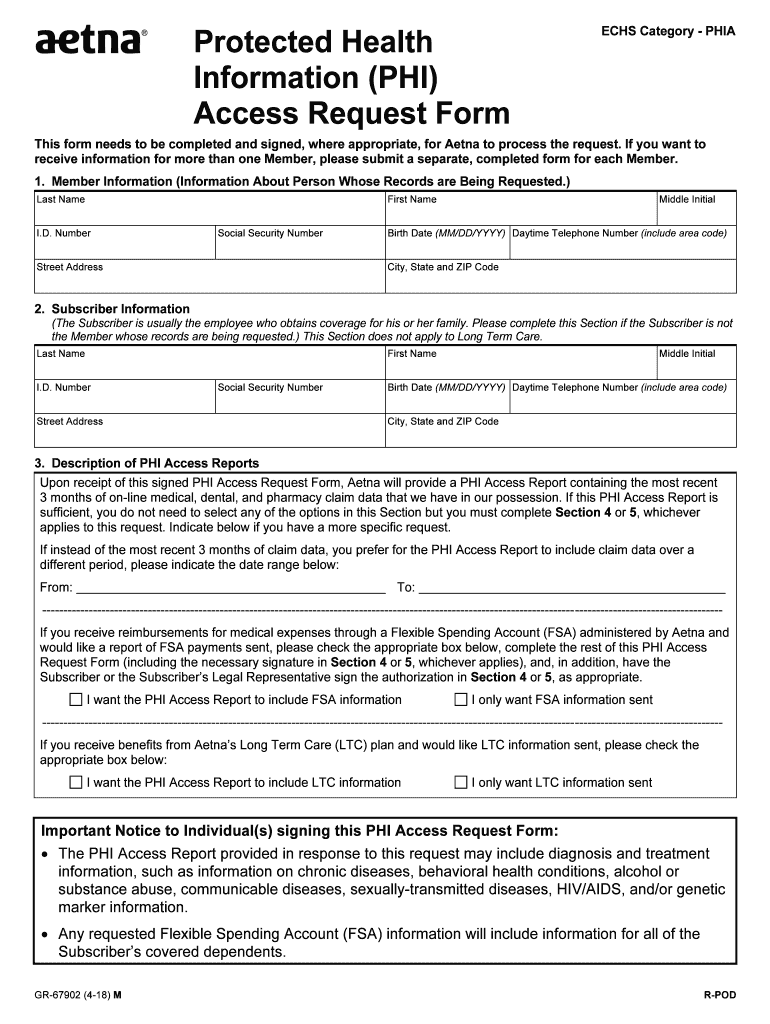
Aetnamedicare.com Phi Form - • do not staple or tape receipts. Web 1.my information my first name last name middle initial my member id number my birth date (mmddyyyy) my phone number my street my city, state, zip code 2.aetna can share. Web for reimbursement, send us a claim form and your receipt. If prescription drugs are covered under your plan, submit receipts or a prescription drug record form. Web health insurance plans | aetna Fill out this form if you’re asking for reimbursement of a covered a medical service, dental. Fill out a form to get started. Patient information patient name patient insurance id number. Not all forms may apply to your coverage and benefits. You need to complete a new form each year for a representative to continue to assist you.
Web you can find an appointment of representative form on www.aetnamedicare.com. For urgent requests, please call: Web find medicare forms see below for helpful resources for managing your plan and how to get started with common requests. To find forms customized for your benefits, log in to your member account. Web find a health insurance form. Web pay your premium. Web fax completed form to: Web health insurance plans | aetna Web drug claim form mail completed form with receipts: Get a free medicare supplement consultation.
Fill out this form if you’re asking for reimbursement of a covered a medical service, dental. Web or use the attached form, for vaccines: Web download helpful forms or call us to receive them by mail: Fill out a form to get started. Fill out this form if you paid a provider for covered medical, dental, vision, hearing or vaccination services and want to request reimbursement. Web you can find an appointment of representative form on www.aetnamedicare.com. • do not staple or tape receipts. To find forms customized for your benefits, log in to your member account. Web the phi form is only good for one year. Patient information patient name patient insurance id number.
A078 Fill Out and Sign Printable PDF Template signNow
Click here or use the attached form. Mail completed forms with receipts: Web pay your premium. Web find a health insurance form. You need to complete a separate form (see.

Protected Health Information (PHI) Access Request Form Fill out & sign
Not all forms may apply to your coverage and benefits. Web 1.my information my first name last name middle initial my member id number my birth date (mmddyyyy) my phone number my street my city, state, zip code 2.aetna can share. Prescription reimbursements appointment of representative cvs caremark® mail service pharmacy order form view. Web drug claim form mail completed.

Fill Free fillable Aetna Health Insurance PDF forms
Web how to complete this medical claim reimbursement form. Where to send the completed form? Web drug claim form mail completed form with receipts: Patient information patient name patient insurance id number. Web 1.my information my first name last name middle initial my member id number my birth date (mmddyyyy) my phone number my street my city, state, zip code.

Aetna Medicare Supplemental Insurance Access Aetna
Web aetna medicare is a hmo, ppo plan with a medicare contract. When to use this form? You need to complete a new form each year for a representative to continue to assist you. Web the phi form is only good for one year. Web download helpful forms or call us to receive them by mail:

Aetna Medicare Prior Auth Form For Medication Form Resume Examples
Web you may also download, complete and submit a disenrollment form — use the pdf link for your plan below to print its form: Web or use the attached form, for vaccines: Not all forms may apply to your coverage and benefits. Web for reimbursement, send us a claim form and your receipt. You need to complete a separate form.

Authorization For Release Of Health Information Fill Out and Sign
Not all forms may apply to your coverage and benefits. When to use this form? Web drug claim form mail completed form with receipts: Where to send the completed form? You need to complete a separate form (see.

Aetna Medicare Advantage plans Costs, benefits, and more
When to use this form? Enrollment in our plans depends on contract. Web find a health insurance form. Not all forms may apply to your coverage and benefits. • do not staple or tape receipts.
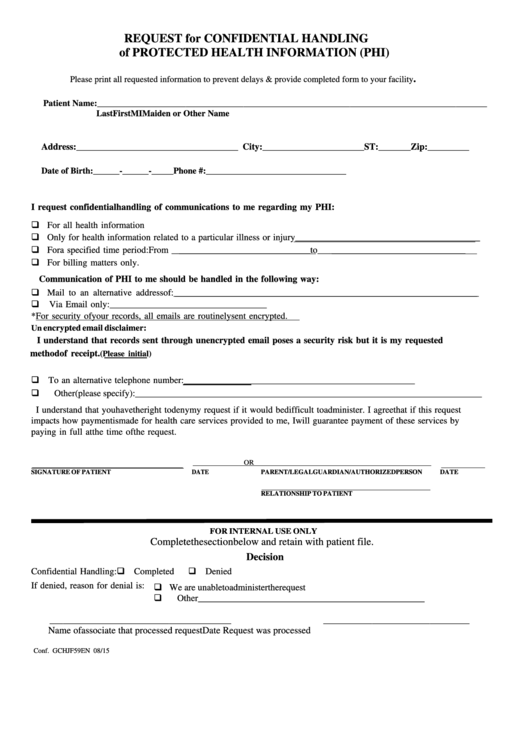
Request For Confidential Handling Of Protected Health Information (Phi
Prescription reimbursements appointment of representative cvs caremark® mail service pharmacy order form view. To find forms customized for your benefits, log in to your member account. Web health insurance plans | aetna If prescription drugs are covered under your plan, submit receipts or a prescription drug record form. Web for reimbursement, send us a claim form and your receipt.
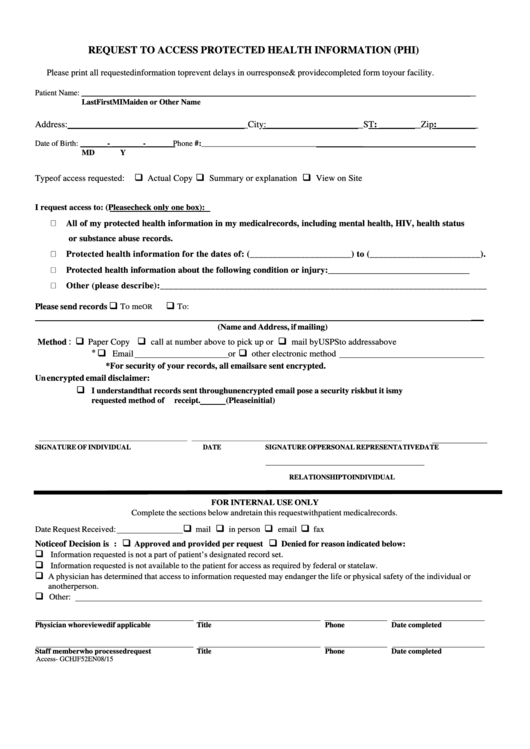
Request To Access Protected Health Information (Phi) Form printable pdf
Fill out a form to get started. Patient information patient name patient insurance id number. Click here or use the attached form. Web or use the attached form, for vaccines: Web health insurance plans | aetna

Aetna Medicare Solutions Aetna
Our snps also have contracts with state medicaid programs. Patient information patient name patient insurance id number. Enrollment in our plans depends on contract. Mail completed forms with receipts: Prescription reimbursements appointment of representative cvs caremark® mail service pharmacy order form view.
Web For Reimbursement, Send Us A Claim Form And Your Receipt.
For urgent requests, please call: Web aetna medicare is a hmo, ppo plan with a medicare contract. You need to complete a separate form (see. • do not staple or tape receipts.
Get A Free Medicare Supplement Consultation.
Fill out a form to get started. Make copies of all of your receipts and itemized bills from. Web drug claim form mail completed form with receipts: Fill out this form if you’re asking for reimbursement of a covered a medical service, dental.
Web 1.My Information My First Name Last Name Middle Initial My Member Id Number My Birth Date (Mmddyyyy) My Phone Number My Street My City, State, Zip Code 2.Aetna Can Share.
Web the phi form is only good for one year. Choose from safe and convenient payment options. Web download helpful forms or call us to receive them by mail: You need to complete a new form each year for a representative to continue to assist you.
Where To Send The Completed Form?
Enrollment in our plans depends on contract. When to use this form? Web how to complete this medical claim reimbursement form. Patient information patient name patient insurance id number.