Cigna Dental Claim Form
Cigna Dental Claim Form - Once you’ve completed the form, print and mail it to one of the following addresses,. This program provides reimbursement for certain eligible dental procedures for customers with qualifying medical conditions. Cigna global health options 1 knowe road greenock pa15 4rj scotland Area of oral cavity 26. Web quickly locate the forms you need for authorizations, referrals, or filing or appealing claims with our forms resource area. You’ll need to upload an itemised treatment receipt showing full details of the treatment carried out and the relevant dates. Log in to cignaforhcp.com to find the dental forms and tools that may be necessary for filing certain claims, appealing claims, and changing information about your office. Customers must enroll in the program prior to receiving dental services to. Missing teeth information (place an “x” on each missing. Web cigna makes it easy for health care providers to submit claims using electronic data interchange (edi).
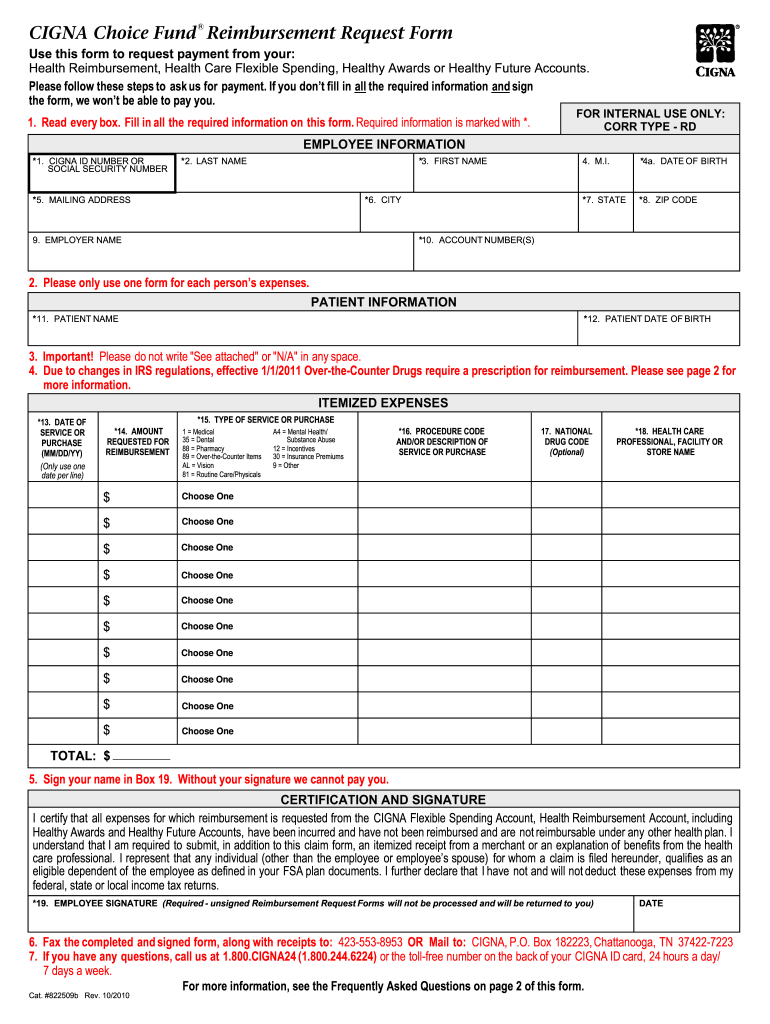
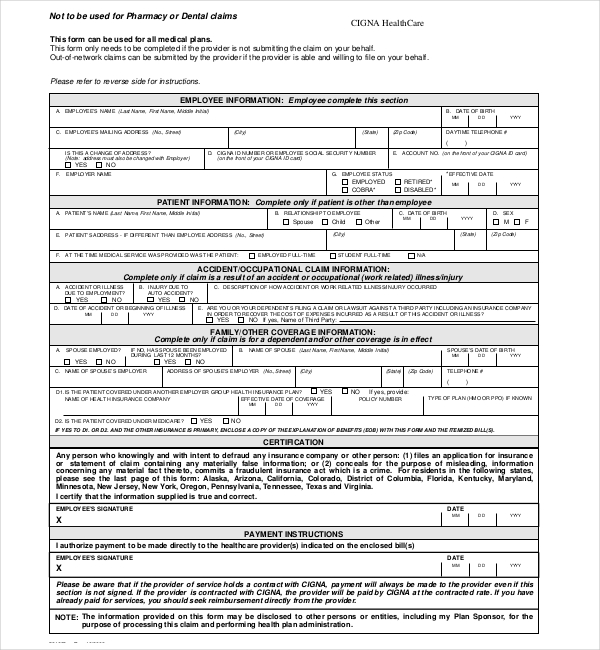
Web the dental oral health integration program. Automate your claims process and save. Tooth number(s) or letter(s) 28. Web dental reimbursement claim form use this form when you want to get reimbursed for a dental benefit that you have already paid for. Web quickly locate the forms you need for authorizations, referrals, or filing or appealing claims with our forms resource area. Treatment incurred inside the usa send to: Treatment incurred outside the usa send to: You’ll need to upload an itemised treatment receipt showing full details of the treatment carried out and the relevant dates. Web login to member portal to submit your dental claim log in to your member portal, click the my claims section and enter your details. Web this section to be completed by the dentist please return your fully completed form along with the original receipt/invoices to:
Log in to cignaforhcp.com to find the dental forms and tools that may be necessary for filing certain claims, appealing claims, and changing information about your office. Missing teeth information (place an “x” on each missing. Fee 1 2 3 4 5 6 7 8 9 10 33. Web quickly locate the forms you need for authorizations, referrals, or filing or appealing claims with our forms resource area. Tooth number(s) or letter(s) 28. Web the dental oral health integration program. Web dental reimbursement claim form use this form when you want to get reimbursed for a dental benefit that you have already paid for. Web this section to be completed by the dentist please return your fully completed form along with the original receipt/invoices to: Cigna global health options 1 knowe road greenock pa15 4rj scotland Web cigna healthcare | health insurance, dental plans & medicare

Cigna Insurance Appeal Fill Online, Printable, Fillable, Blank
We may ask you to complete a claim form if we need more information about your claim. Missing teeth information (place an “x” on each missing. Area of oral cavity 26. Once you’ve completed the form, print and mail it to one of the following addresses,. Treatment incurred inside the usa send to:

Cigna Claim Form Wire Transfer Cheque
Once you’ve completed the form, print and mail it to one of the following addresses,. Web this section to be completed by the dentist please return your fully completed form along with the original receipt/invoices to: Log in to cignaforhcp.com to find the dental forms and tools that may be necessary for filing certain claims, appealing claims, and changing information.
Neuron Cigna Reimbursement Form Fill Online, Printable, Fillable
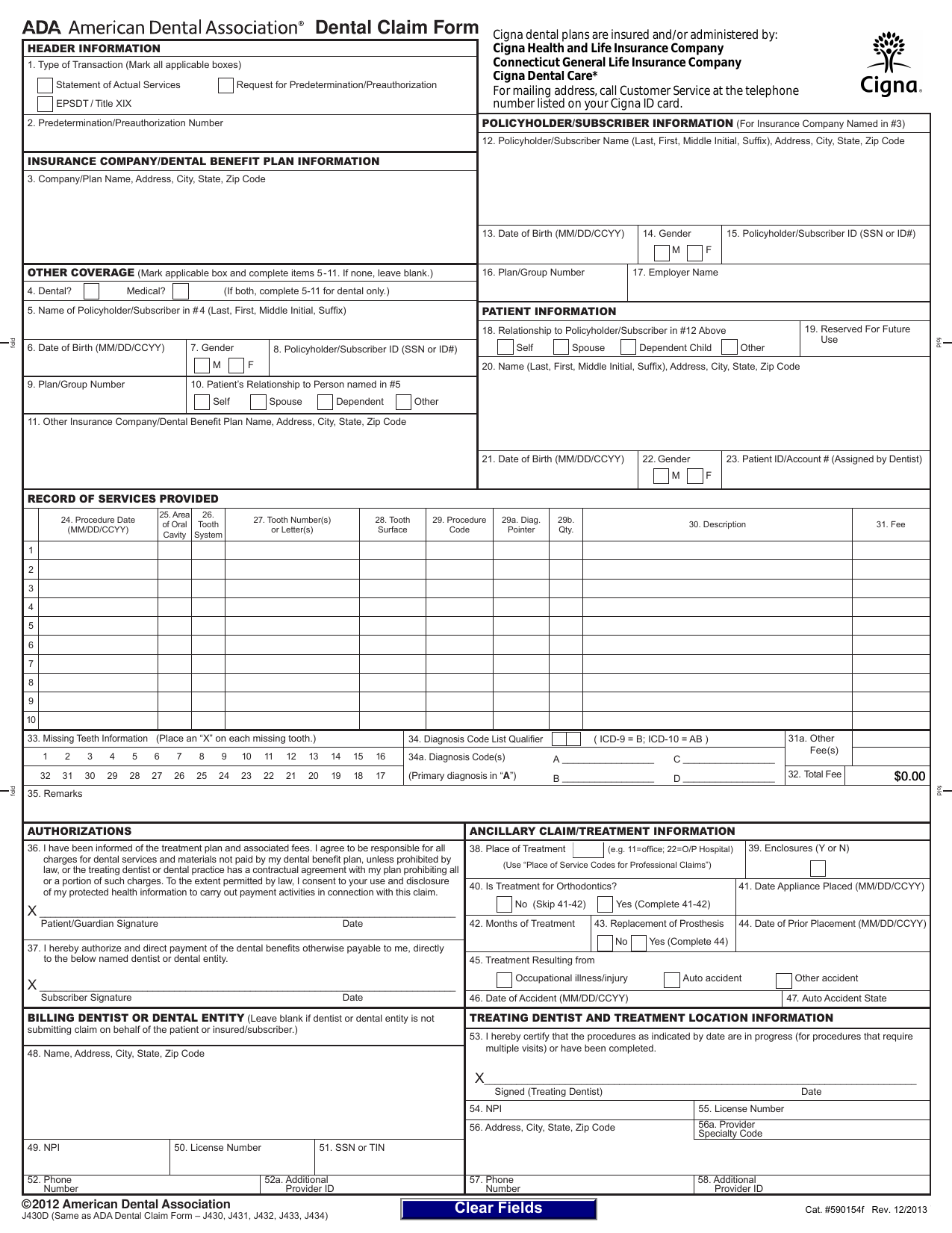
Web this section to be completed by the dentist please return your fully completed form along with the original receipt/invoices to: Missing teeth information (place an “x” on each missing. Treatment incurred outside the usa send to: Tooth number(s) or letter(s) 28. Web 590154f dental claim form cigna record of services provided 24.

Dental Care Claim Form 2010 Cigna Cheque
Automate your claims process and save. Fee 1 2 3 4 5 6 7 8 9 10 33. Once you’ve completed the form, print and mail it to one of the following addresses,. Customers must enroll in the program prior to receiving dental services to. Missing teeth information (place an “x” on each missing.

Cigna Uft Dental Claim form Elegant Co Op City Times 05 08 10 by Co Op
Log in to cignaforhcp.com to find the dental forms and tools that may be necessary for filing certain claims, appealing claims, and changing information about your office. Web this section to be completed by the dentist please return your fully completed form along with the original receipt/invoices to: Customers must enroll in the program prior to receiving dental services to..
Download CIGNA Dental Claim Form J430D PDF RTF Word
Web cigna healthcare | health insurance, dental plans & medicare Web this section to be completed by the dentist please return your fully completed form along with the original receipt/invoices to: This program provides reimbursement for certain eligible dental procedures for customers with qualifying medical conditions. Treatment incurred inside the usa send to: Once you’ve completed the form, print and.

Sell Cigna Dental, Vision, and Hearing Insurance New Horizons
Web the dental oral health integration program. Treatment incurred outside the usa send to: You’ll need to upload an itemised treatment receipt showing full details of the treatment carried out and the relevant dates. Fee 1 2 3 4 5 6 7 8 9 10 33. Web cigna healthcare | health insurance, dental plans & medicare
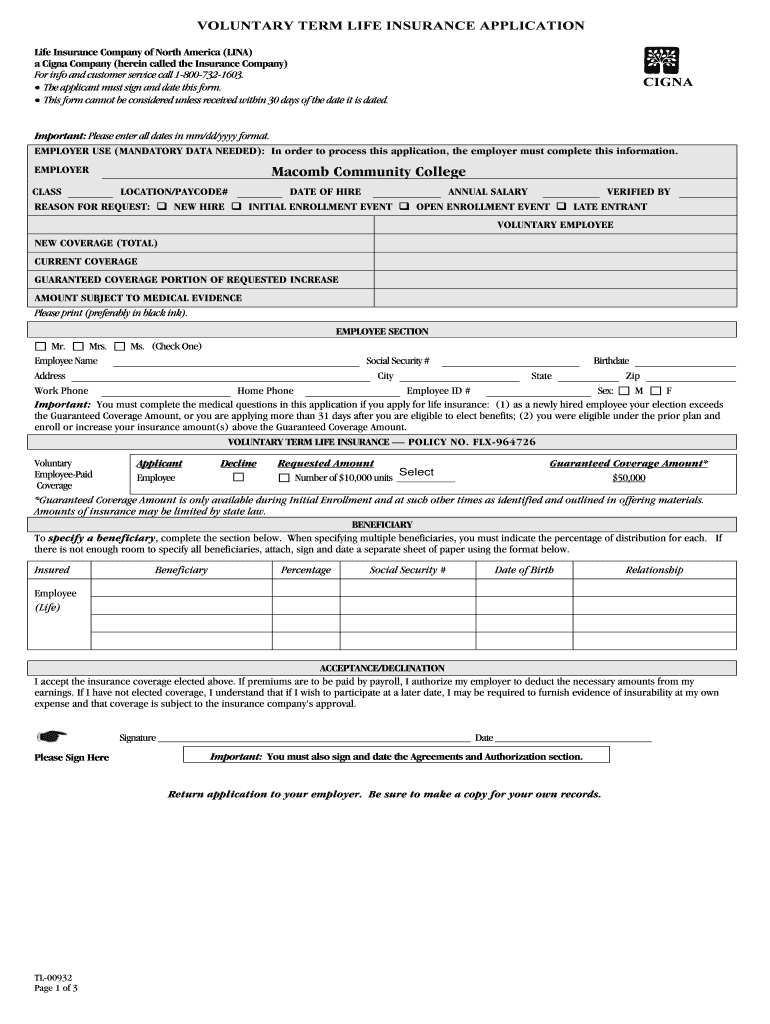
Cigna TL00932 Fill and Sign Printable Template Online US Legal Forms
Web the dental oral health integration program. You’ll need to upload an itemised treatment receipt showing full details of the treatment carried out and the relevant dates. This program provides reimbursement for certain eligible dental procedures for customers with qualifying medical conditions. Fee 1 2 3 4 5 6 7 8 9 10 33. Once you’ve completed the form, print.

Cigna MBA Claim Form_505808707 Cigna Wire Transfer
Web cigna healthcare | health insurance, dental plans & medicare Web this section to be completed by the dentist please return your fully completed form along with the original receipt/invoices to: Treatment incurred outside the usa send to: Web login to member portal to submit your dental claim log in to your member portal, click the my claims section and.
FREE 11+ Sample Medical Claim Forms in PDF MS Word Excel
Web cigna makes it easy for health care providers to submit claims using electronic data interchange (edi). Tooth number(s) or letter(s) 28. Web 590154f dental claim form cigna record of services provided 24. Fee 1 2 3 4 5 6 7 8 9 10 33. Automate your claims process and save.
Web Cigna Healthcare | Health Insurance, Dental Plans & Medicare
Customers must enroll in the program prior to receiving dental services to. Web login to member portal to submit your dental claim log in to your member portal, click the my claims section and enter your details. We may ask you to complete a claim form if we need more information about your claim. Web 590154f dental claim form cigna record of services provided 24.
Area Of Oral Cavity 26.
Treatment incurred inside the usa send to: Web cigna makes it easy for health care providers to submit claims using electronic data interchange (edi). Tooth number(s) or letter(s) 28. You’ll need to upload an itemised treatment receipt showing full details of the treatment carried out and the relevant dates.
Fee 1 2 3 4 5 6 7 8 9 10 33.
This program provides reimbursement for certain eligible dental procedures for customers with qualifying medical conditions. Web quickly locate the forms you need for authorizations, referrals, or filing or appealing claims with our forms resource area. Automate your claims process and save. Cigna global health options 1 knowe road greenock pa15 4rj scotland
Treatment Incurred Outside The Usa Send To:
Log in to cignaforhcp.com to find the dental forms and tools that may be necessary for filing certain claims, appealing claims, and changing information about your office. Web this section to be completed by the dentist please return your fully completed form along with the original receipt/invoices to: Missing teeth information (place an “x” on each missing. Once you’ve completed the form, print and mail it to one of the following addresses,.