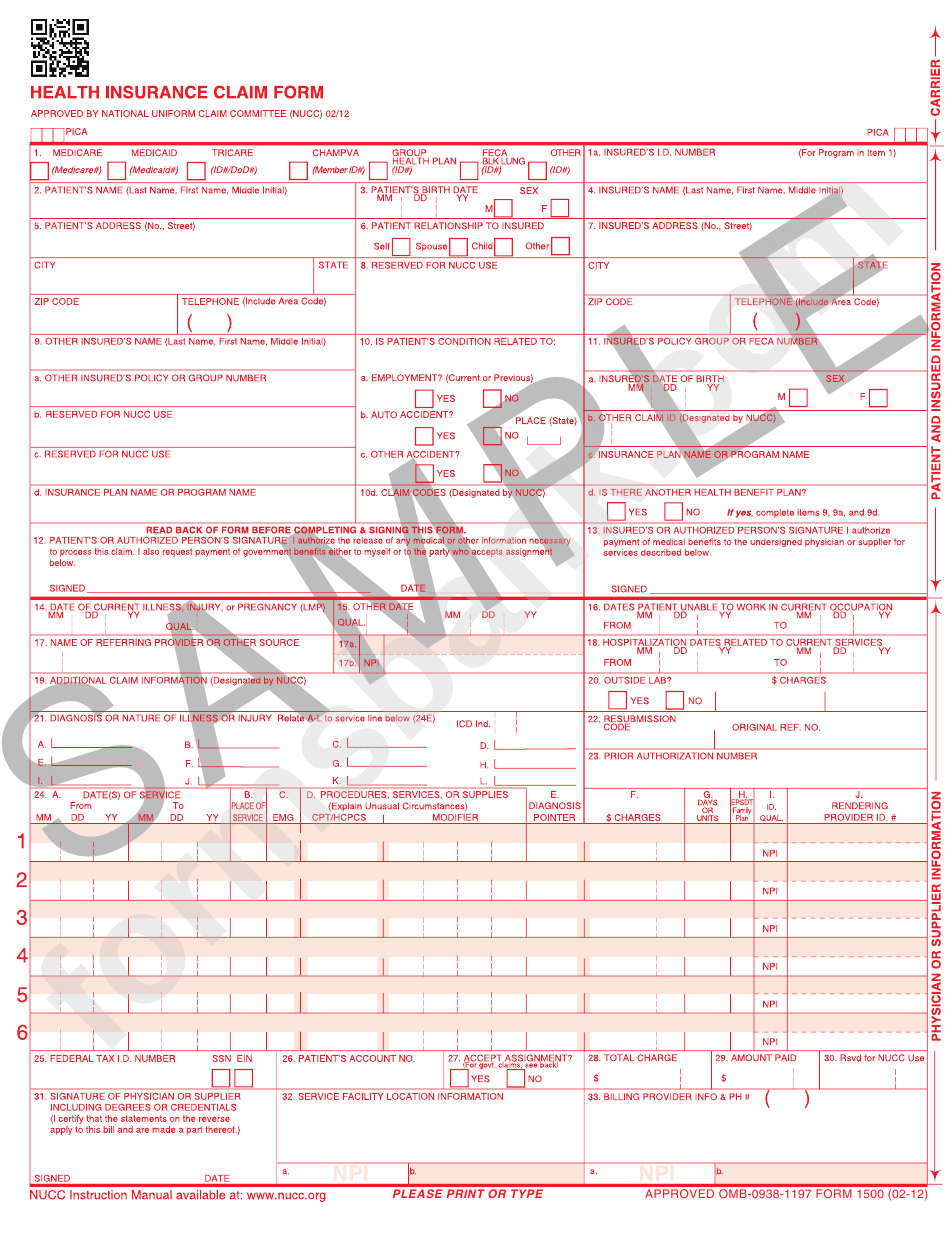
Cms 1500 Claim Form Sample
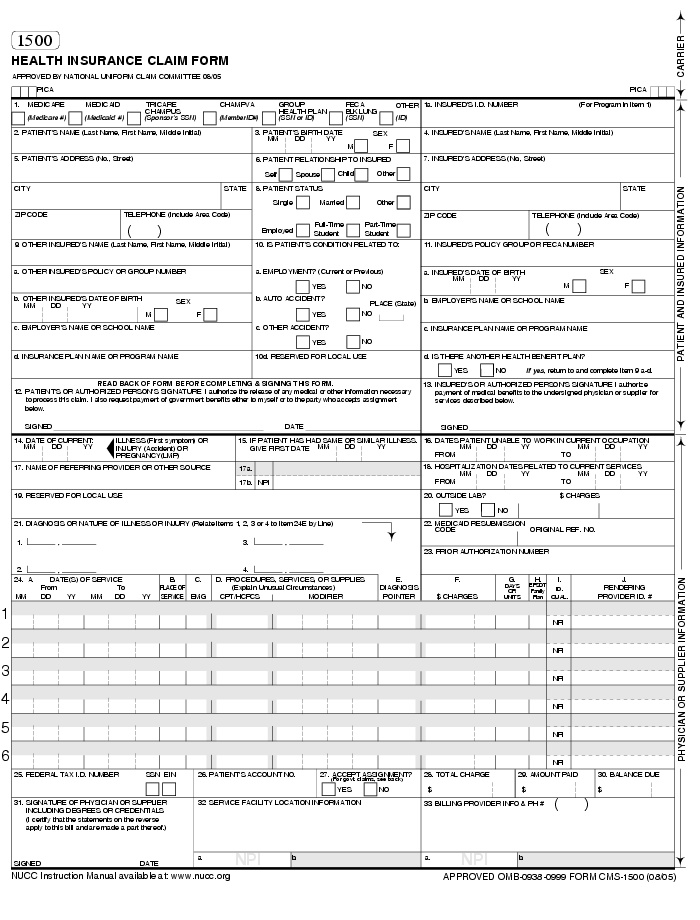
Cms 1500 Claim Form Sample - It is also used for submitting claims to many. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. New cms1500 claim form tenn med. Health insurance claim form 1. In the case of a medicare claim, the patient’s signature authorizes any entity to release to medicare medical and nonmedical information, including employment status, and whether the person has employer group health The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. 17124907 mesh terms forms and records control humans insurance claim reporting* united states. You can decide how often to. Single sheet claim forms suitable for either ink jet or laser printers. It can be purchased in any version required by calling the u.s.
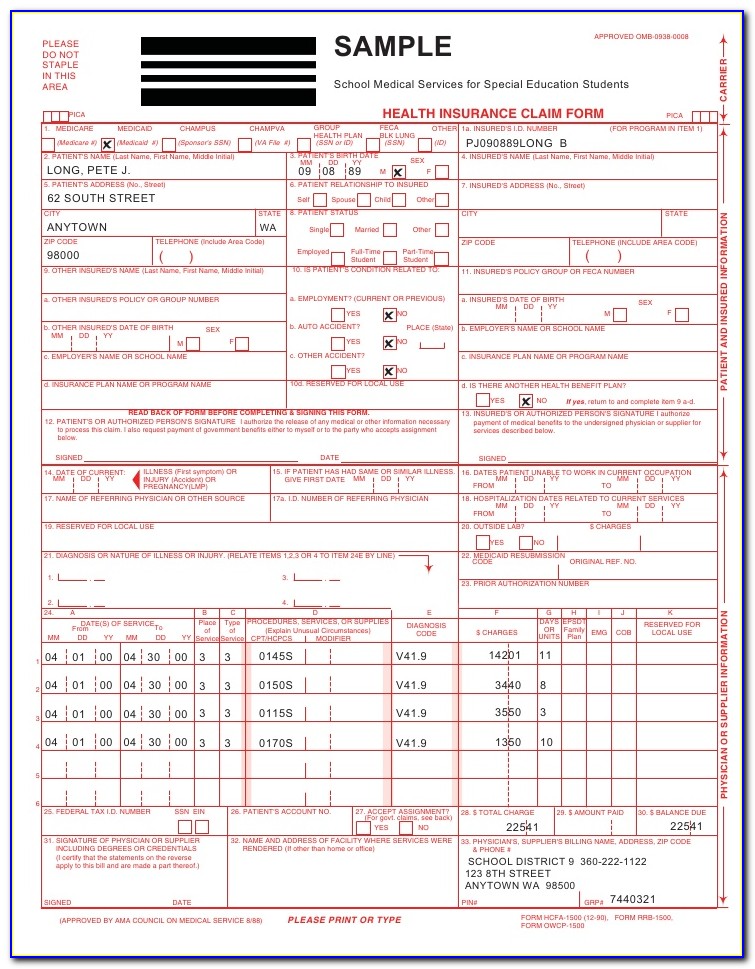
Web cms 1500 dynamic list information. I also request payment of. It is available in various formats (e.g., single copy, duplicate, etc.). The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Health insurance claim form 1. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. Web billing tips when completing claims, do not enter the decimal point in any codes or dollar amounts. Last updated wed, 04 jan 2023 13:36:02 +0000. Web new cms1500 claim form. The patient was seen for an office visit (99213).
In the case of a medicare claim, the patient’s signature authorizes any entity to release to medicare medical and nonmedical information, including employment status, and whether the person has employer group health Medicare medicaid tricare champva other read back of form before completing & signing this form. I also request payment of. Web cms 1500 dynamic list information. You'll see instructions on how to complete the field. New cms1500 claim form tenn med. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Insured’s name (last name, first name, middle initial).
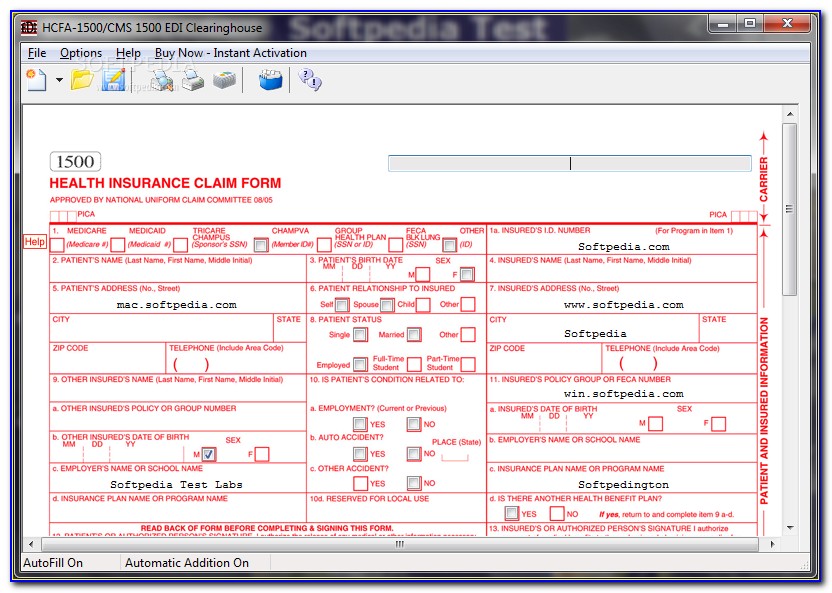
Form Cms1500 Health Insurance Claim Form Sample printable pdf download
The patient was seen for an office visit (99213). It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim. Insured’s name (last name,.

Cms 1500 Claim Form Pdf Free Download Forms OTM0NA Resume Examples
Health insurance claim form 1. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services. Insured’s name (last name, first name, middle initial). Sign up to get the latest information about your choice of cms topics. Web health insurance claim form 1.
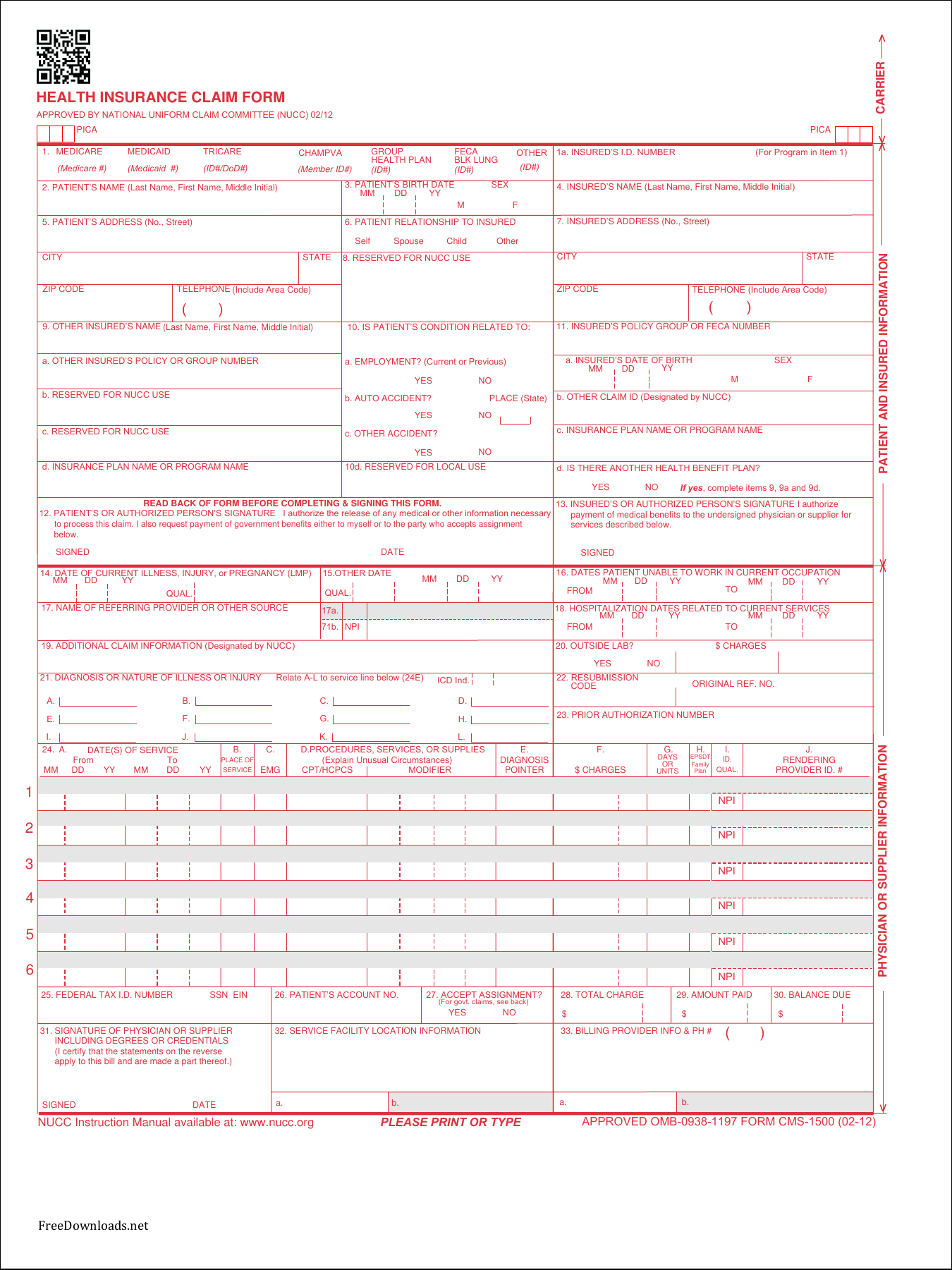
Completed Cms 1500 Claim Form Sample Form Resume Examples K75PBGVkl2
You may also click in any field for more detailed instructions. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services. Web the claim and certifies that the information provided in blocks 1 through 12 is true, accurate and complete. It can be.

Cms 1500 Claim Form Instructions 2016 Form Resume Examples XE8je6e3Oo
Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Insured’s name (last name,.
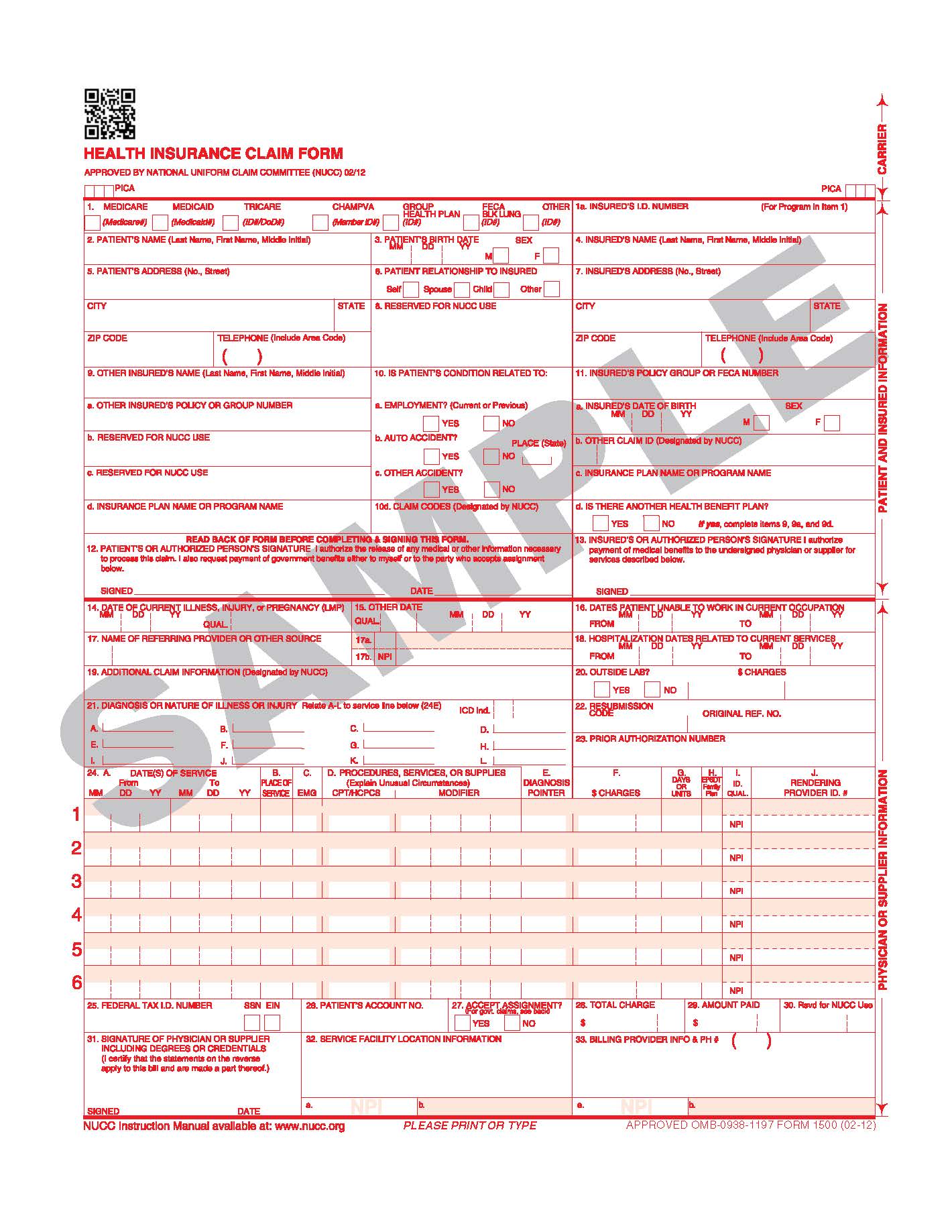
Download Fillable CMS Claim Form 1500 PDF
It is available in various formats (e.g., single copy, duplicate, etc.). Web cms 1500 dynamic list information. Number (for program in item 1) 4. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by.
Changes to the 1500 Claim Form Healthcare Data Management
Web new cms1500 claim form. It can be purchased in any version required by calling the u.s. Web the claim and certifies that the information provided in blocks 1 through 12 is true, accurate and complete. You may also click in any field for more detailed instructions. Forms are completely compliant with the medicare specifications.

Cms 1500 Claim Form Pdf Forms NDA3NA Resume Examples
The provider is reporting several measures related to diabetes, coronary artery disease (cad), and urinary incontinence: Medicare medicaid champus champva other read back of form before completing & signing this form. You may also click in any field for more detailed instructions. Web health insurance claim form 1. Number (for program in item 1) 4.
cms claimbilling CMS 1500 claim form billing instruction Part 3
Number (for program in item 1) 4. New cms1500 claim form tenn med. Sign up to get the latest information about your choice of cms topics. Single sheet claim forms suitable for either ink jet or laser printers. Web new cms1500 claim form.
Blank Ub 04 Claim Form Form Resume Examples rykgPYKDwn
You can decide how often to. Sign up to get the latest information about your choice of cms topics. Web cms 1500 dynamic list information. Last updated wed, 04 jan 2023 13:36:02 +0000. Health insurance claim form 1.

cms1500claimformsample CASO Document Management
You may also click in any field for more detailed instructions. Web new cms1500 claim form. The provider is reporting several measures related to diabetes, coronary artery disease (cad), and urinary incontinence: Single sheet claim forms suitable for either ink jet or laser printers. Medicare medicaid tricare champva other read back of form before completing & signing this form.
Web The Claim And Certifies That The Information Provided In Blocks 1 Through 12 Is True, Accurate And Complete.
The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Forms are completely compliant with the medicare specifications. Single sheet claim forms suitable for either ink jet or laser printers. In the case of a medicare claim, the patient’s signature authorizes any entity to release to medicare medical and nonmedical information, including employment status, and whether the person has employer group health
Number (For Program In Item 1) 4.
Insured’s name (last name, first name, middle initial). Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. I also request payment of. You can decide how often to.
17124907 Mesh Terms Forms And Records Control Humans Insurance Claim Reporting* United States.
The patient was seen for an office visit (99213). It can be purchased in any version required by calling the u.s. It is also used for submitting claims to many. Last updated wed, 04 jan 2023 13:36:02 +0000.
New Cms1500 Claim Form Tenn Med.
Web billing tips when completing claims, do not enter the decimal point in any codes or dollar amounts. Web cms 1500 dynamic list information. You may also click in any field for more detailed instructions. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary to process this claim.