Hmsa Prior Authorization Form
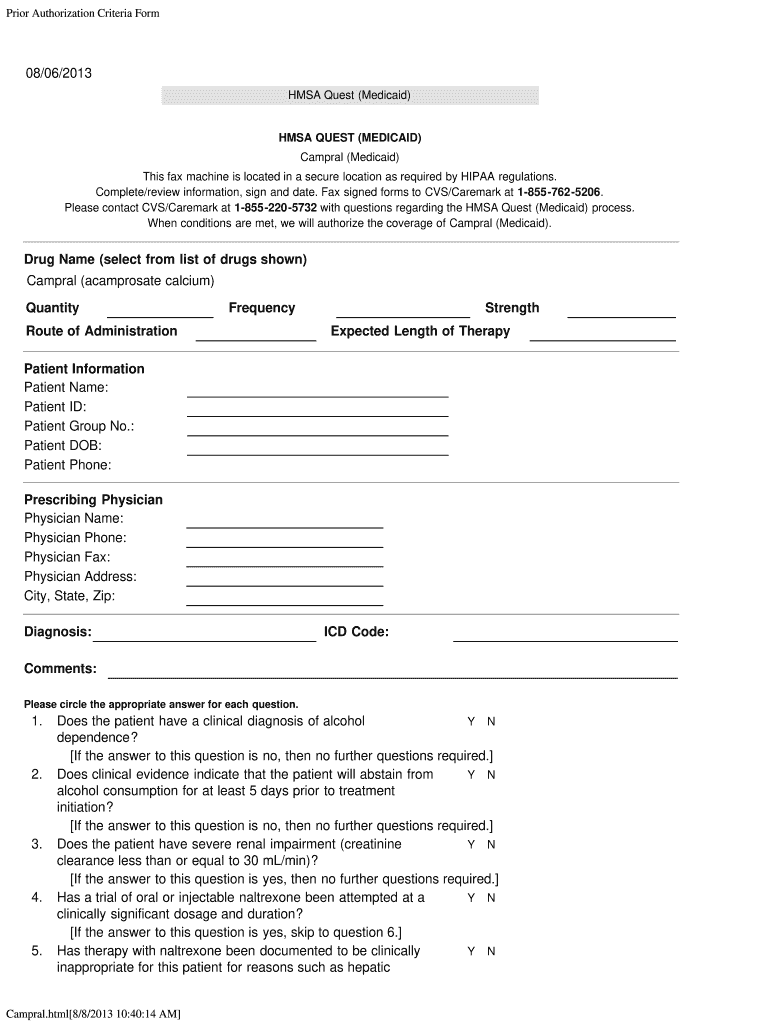
Hmsa Prior Authorization Form - This standardized form is used for a general request for hmsa all lines of business when no other precertification request form applies. _ patient information last name first name phone number gender m f date of birth member id # (if known): Hmsa medical management department p. Decision & notification are made within 14calendar days* for hmsa commercial, federal and eutf plans: To make an appropriate determination, providing the most accurate diagnosis for the use of the prescribed medication is necessary. Web this standardized prior authorization request form can be used for most prior authorization requests and use across all four health plans, including alohacare, hmsa, 'ohana health plan, and united healthcare. Fast pass providers aren’t required to request prior authorization. Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. To make an appropriate determination, providing the most accurate diagnosis for the use of the Web standard request for medicare and medicaid plans:
Requesting prior authorization • providers are encouraged to use radmd.com to request prior authorization. Decisions & notification are made within 15calendar days* expedited request (md,. This standardized form is used for a general request for hmsa all lines of business when no other precertification request form applies. This patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. Fast pass providers aren’t required to request prior authorization. Contact name (first, last) member. Decision & notification are made within 14calendar days* for hmsa commercial, federal and eutf plans: Web utilization management (um) department prior authorization request phone number: To make an appropriate determination, providing the most accurate diagnosis for the use of the To make an appropriate determination, providing the most accurate diagnosis for the use of the prescribed medication is necessary.
Web this standardized prior authorization request form can be used for most prior authorization requests and use across all four health plans, including alohacare, hmsa, 'ohana health plan, and united healthcare. This standardized form is used for a general request for hmsa all lines of business when no other precertification request form applies. _ patient information last name first name phone number gender m f date of birth member id # (if known): Hmsa medical management department p. Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. Requesting prior authorization • providers are encouraged to use radmd.com to request prior authorization. This patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. To make an appropriate determination, providing the most accurate diagnosis for the use of the Web standard request for medicare and medicaid plans: To make an appropriate determination, providing the most accurate diagnosis for the use of the prescribed medication is necessary.
Authorization Medicaid Campral Fill Out and Sign Printable PDF
Decisions & notification are made within 15calendar days* expedited request (md,. Hmsa medical management department p. Requesting prior authorization • providers are encouraged to use radmd.com to request prior authorization. _ patient information last name first name phone number gender m f date of birth member id # (if known): This patient’s benefit plan requires prior authorization for certain medications.
Ach Payment Authorization Form Template Template 2 Resume Examples
Contact name (first, last) member. _ patient information last name first name phone number gender m f date of birth member id # (if known): Web this standardized prior authorization request form can be used for most prior authorization requests and use across all four health plans, including alohacare, hmsa, 'ohana health plan, and united healthcare. To make an appropriate.

REQUEST FOR MEDICAL AUTHORIZATION in Word and Pdf formats
To make an appropriate determination, providing the most accurate diagnosis for the use of the Web utilization management (um) department prior authorization request phone number: To make an appropriate determination, providing the most accurate diagnosis for the use of the prescribed medication is necessary. Fast pass providers aren’t required to request prior authorization. Decisions & notification are made within 15calendar.
FREE 8+ Sample Prior Authorization Forms in PDF MS Word
Web utilization management (um) department prior authorization request phone number: Hmsa medical management department p. To make an appropriate determination, providing the most accurate diagnosis for the use of the Decisions & notification are made within 15calendar days* expedited request (md,. This patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered.
FREE 13+ Prior Authorization Forms in PDF MS Word
Fast pass providers aren’t required to request prior authorization. This patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. Decisions & notification are made within 15calendar days* expedited request (md,. Decision & notification are made within 14calendar days* for hmsa commercial, federal and eutf plans: Web utilization management (um) department prior authorization.

Hmsa Medicaid Form Request Fill Online, Printable, Fillable, Blank
Web standard request for medicare and medicaid plans: Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. Hmsa medical management department p. To make an appropriate determination, providing the most accurate diagnosis for the use of the prescribed medication is necessary. _ patient information last name first name phone number.
Hmsa Membership Report Form Fill Out and Sign Printable PDF Template
Web utilization management (um) department prior authorization request phone number: Hmsa medical management department p. This patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. Web hawaii medicaid prior authorization form hawaii standardized prescription drug prior authorization form* request date: To make an appropriate determination, providing the most accurate diagnosis for the.

ads/responsive.txt Health Net Prior Authorization form for Medication
Web hawaii medicaid prior authorization form hawaii standardized prescription drug prior authorization form* request date: Decision & notification are made within 14calendar days* for hmsa commercial, federal and eutf plans: Decisions & notification are made within 15calendar days* expedited request (md,. Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered..

Medco Prior Authorization Form Form Resume Examples XV8oMxYKzD
Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. This standardized form is used for a general request for hmsa all lines of business when no other precertification request form applies. Web standard request for medicare and medicaid plans: Web this standardized prior authorization request form can be used for.

Express Scripts Prior Authorization Form Medicare Part D Form
This patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. _ patient information last name first name phone number gender m f date of birth member id # (if known): Web this standardized prior authorization request form can be used for most prior authorization requests and use across all four health plans,.
_ Patient Information Last Name First Name Phone Number Gender M F Date Of Birth Member Id # (If Known):
Decisions & notification are made within 15calendar days* expedited request (md,. This patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. This standardized form is used for a general request for hmsa all lines of business when no other precertification request form applies. Fast pass providers aren’t required to request prior authorization.
To Make An Appropriate Determination, Providing The Most Accurate Diagnosis For The Use Of The
Contact name (first, last) member. Web standard request for medicare and medicaid plans: Web this standardized prior authorization request form can be used for most prior authorization requests and use across all four health plans, including alohacare, hmsa, 'ohana health plan, and united healthcare. This patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered.
Web Utilization Management (Um) Department Prior Authorization Request Phone Number:
Hmsa medical management department p. Decision & notification are made within 14calendar days* for hmsa commercial, federal and eutf plans: Requesting prior authorization • providers are encouraged to use radmd.com to request prior authorization. Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered.
Web Hawaii Medicaid Prior Authorization Form Hawaii Standardized Prescription Drug Prior Authorization Form* Request Date:
To make an appropriate determination, providing the most accurate diagnosis for the use of the prescribed medication is necessary.