Home Health Plan Of Care Form
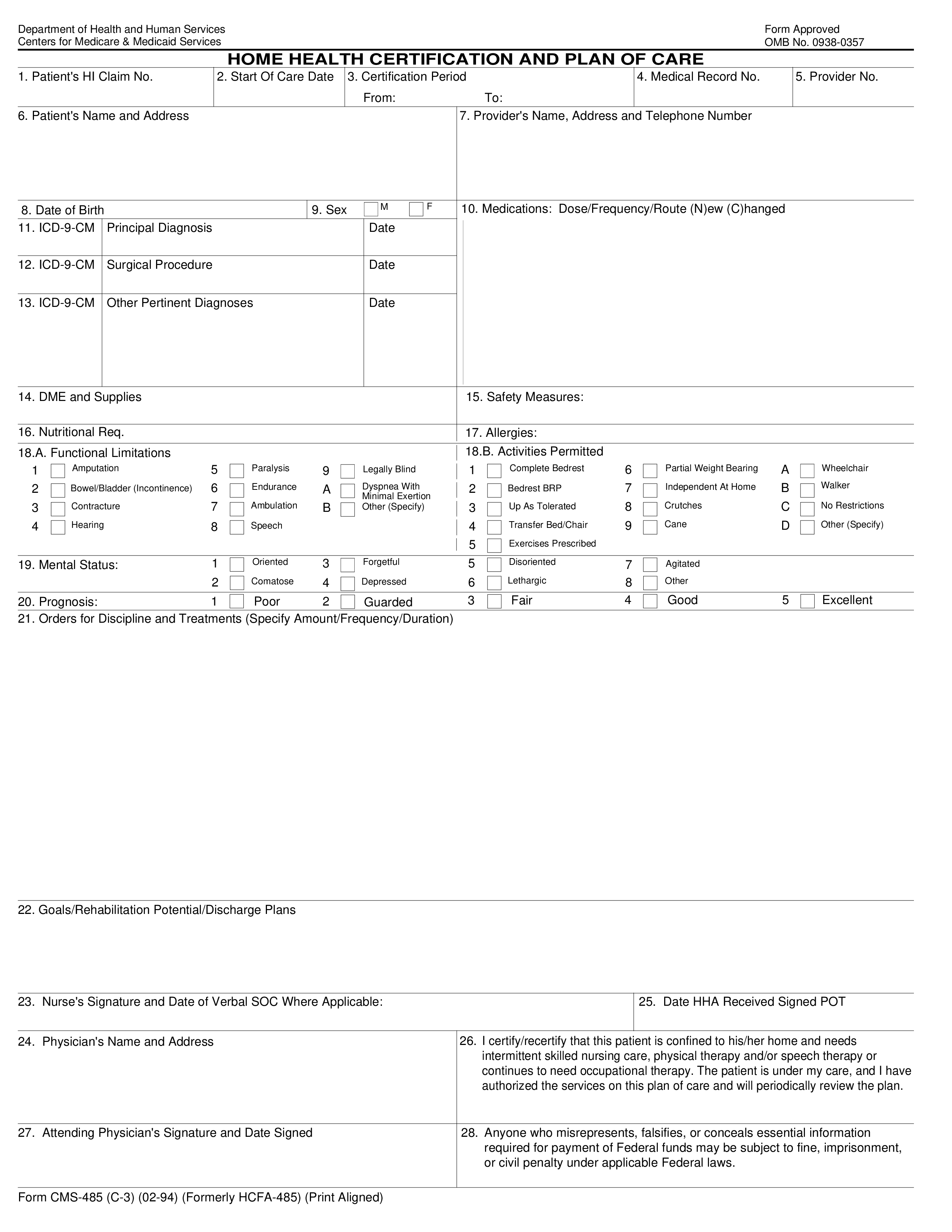
Home Health Plan Of Care Form - Patient's name and address 7. Start of care date 3. Web this template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the medicare beneficiary’s eligibility and need for home health services. Web home health certification and plan of care. Or suggestions for improving this form, please write to: Start of care date 3. Provider's name, address and telephone number 4. Patient's name and address 7. The provider and prior authorization request submitter certify and affirm that they understand and agree that prior authorization is a condition of reimbursement and is not a guarantee of payment. Web home health certification and plan of care 1.
Care planning, coordination of services, and quality of care, requires that. Start of care date 3. Web home health certification and plan of care 1. Provider's name, address and telephone number 4. Web your home health agency must give you or arrange for all the home care listed in your plan of care, including services and medical supplies. Web this template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the medicare beneficiary’s eligibility and need for home health services. Start of care date 3. Use this free home health certification and plan of care form template to sign patients. The provider and prior authorization request submitter certify and affirm that they understand and agree that prior authorization is a condition of reimbursement and is not a guarantee of payment. Start of care date 3.
Start of care date 3. Provider's name, address and telephone number 4. Start of care date 3. Web home health certification and plan of care. Web this template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the medicare beneficiary’s eligibility and need for home health services. 42 cfr 484.60, condition of participation: The provider and prior authorization request submitter certify and affirm that they understand and agree that prior authorization is a condition of reimbursement and is not a guarantee of payment. Web texas medicaid provider procedures manual (tmppm). Web home health certification and plan of care 1. Your doctor or allowed practitioner and home health team should review your plan of care as often as.

free printable templates for nursing care plans Google Search
Patient's name and address 7. Use this free home health certification and plan of care form template to sign patients. Web home health certification and plan of care 1. Patient's name and address 7. Care planning, coordination of services, and quality of care, requires that.
Home Health Care Plan Templates at
Web a home health certification and plan of care form is a legal agreement used by home health agencies to sign up patients for home health care. Provider's name, address and telephone number 4. Patient's name and address 7. Patient's name and address 7. Or suggestions for improving this form, please write to:
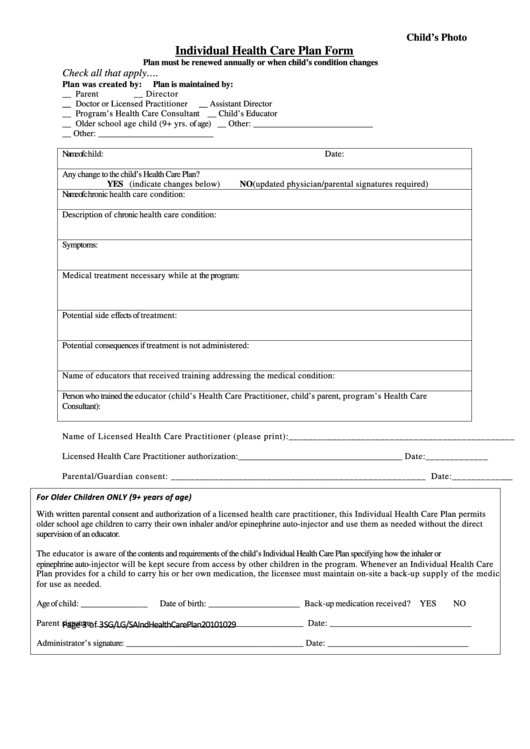
Individual Health Care Plan Form printable pdf download
Web home health certification and plan of care. Start of care date 3. Web home health certification and plan of care 1. 42 cfr 484.60, condition of participation: Web a home health certification and plan of care form is a legal agreement used by home health agencies to sign up patients for home health care.

Addictionary
Provider's name, address and telephone number 4. Web home health certification and plan of care 1. Web home health certification and plan of care. Web this template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the medicare beneficiary’s eligibility and need for home health services. Start of care.

Addictionary
Start of care date 3. The provider and prior authorization request submitter certify and affirm that they understand and agree that prior authorization is a condition of reimbursement and is not a guarantee of payment. 42 cfr 484.60, condition of participation: Your doctor or allowed practitioner and home health team should review your plan of care as often as. Care.
8 Plan Of Care Template Perfect Template Ideas
Patient's name and address 7. Start of care date 3. Web home health certification and plan of care 1. Your doctor or allowed practitioner and home health team should review your plan of care as often as. Web your home health agency must give you or arrange for all the home care listed in your plan of care, including services.
15 Best Images of Health & Nutrition Worksheets Mental Health Quote
Provider's name, address and telephone number 4. Web your home health agency must give you or arrange for all the home care listed in your plan of care, including services and medical supplies. 42 cfr 484.60, condition of participation: Web home health certification and plan of care 1. Care planning, coordination of services, and quality of care, requires that.

Plan of Care Template 2 Free Templates in PDF, Word, Excel Download
Start of care date 3. Web your home health agency must give you or arrange for all the home care listed in your plan of care, including services and medical supplies. Web this template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the medicare beneficiary’s eligibility and need.

Home Health Care Plan Template Awesome 10 Best Of Care now Doctors Note
Patient's name and address 7. Web a home health certification and plan of care form is a legal agreement used by home health agencies to sign up patients for home health care. Provider's name, address and telephone number 4. 42 cfr 484.60, condition of participation: Care planning, coordination of services, and quality of care, requires that.

Nursing Home Care Plan Template Awesome Home Nursing Care Plan Sample
Web home health certification and plan of care 1. Or suggestions for improving this form, please write to: Web a home health certification and plan of care form is a legal agreement used by home health agencies to sign up patients for home health care. Web your home health agency must give you or arrange for all the home care.
Your Doctor Or Allowed Practitioner And Home Health Team Should Review Your Plan Of Care As Often As.
Web home health certification and plan of care. The provider and prior authorization request submitter certify and affirm that they understand and agree that prior authorization is a condition of reimbursement and is not a guarantee of payment. Start of care date 3. Web texas medicaid provider procedures manual (tmppm).
Web Your Home Health Agency Must Give You Or Arrange For All The Home Care Listed In Your Plan Of Care, Including Services And Medical Supplies.
42 cfr 484.60, condition of participation: Care planning, coordination of services, and quality of care, requires that. Patient's name and address 7. Web home health certification and plan of care 1.
Web Home Health Certification And Plan Of Care 1.
Start of care date 3. Or suggestions for improving this form, please write to: Use this free home health certification and plan of care form template to sign patients. Start of care date 3.
Web A Home Health Certification And Plan Of Care Form Is A Legal Agreement Used By Home Health Agencies To Sign Up Patients For Home Health Care.
Provider's name, address and telephone number 4. You can use the clinical templates or suggested clinical data elements (cdes) to. Provider's name, address and telephone number 4. Web this template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the medicare beneficiary’s eligibility and need for home health services.