Income Verification Form Dcf
Income Verification Form Dcf - We need specific amounts to determine eligibility. Office address / phone number: Web case name _____ case number/cat/seq. Case name:___________________________________________ case number:___________________ month:___________________ for every day you work,. § 435,910, el departamento está solicitando proporcionarle el número de seguro social (ssn), pero no es necesario que nos proporcione el número de seguro social bajo la ley. Any person who intentionally fails to give accurate information may be subject to prosecution for fraud. Some forms require adobe acrobat. Hearings request for public assistance. Web include details of your business’s income and expenses for the past three months and upload the completed form to your application. Verification of employment/loss of income.
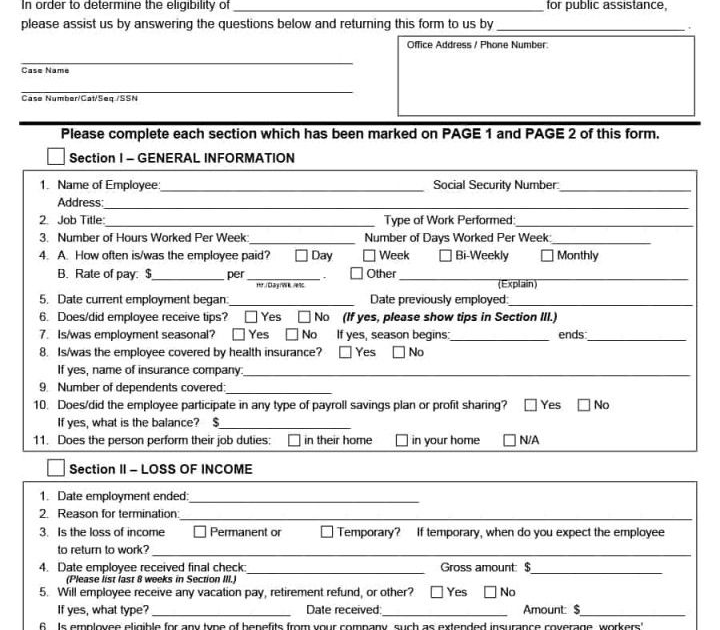
Web case name _____ case number/cat/seq. Any person who intentionally fails to give accurate information may be subject to prosecution for fraud. Name:_______________________________ ssn:______________________ id number:______________________ s ection i: When completing this form please do not use phrases such as “amount varies”, “it varies from month to month”, or “as much as i can”. Web include details of your business’s income and expenses for the past three months and upload the completed form to your application. Web income verification request to: § 435,910, el departamento está solicitando proporcionarle el número de seguro social (ssn), pero no es necesario que nos proporcione el número de seguro social bajo la ley. The following provide links to every form and application that governs the licensing, registration, training and accreditation processes of child care facilities and homes within the state of florida. Please complete each section which has been marked on page 1 and page 2 of this form. We need specific amounts to determine eligibility.
When completing this form please do not use phrases such as “amount varies”, “it varies from month to month”, or “as much as i can”. Case name:___________________________________________ case number:___________________ month:___________________ for every day you work,. Any person who intentionally fails to give accurate information may be subject to prosecution for fraud. The following provide links to every form and application that governs the licensing, registration, training and accreditation processes of child care facilities and homes within the state of florida. Web case name _____ case number/cat/seq. Verification of employment/loss of income. Web de conformidad con el 42 c.f.r. Please complete each section which has been marked on page 1 and page 2 of this form. Agency request the above named individual has applied for assistance from the state of florida. Web include details of your business’s income and expenses for the past three months and upload the completed form to your application.

30 Previous Employment Verification form Template (2020) Letter of
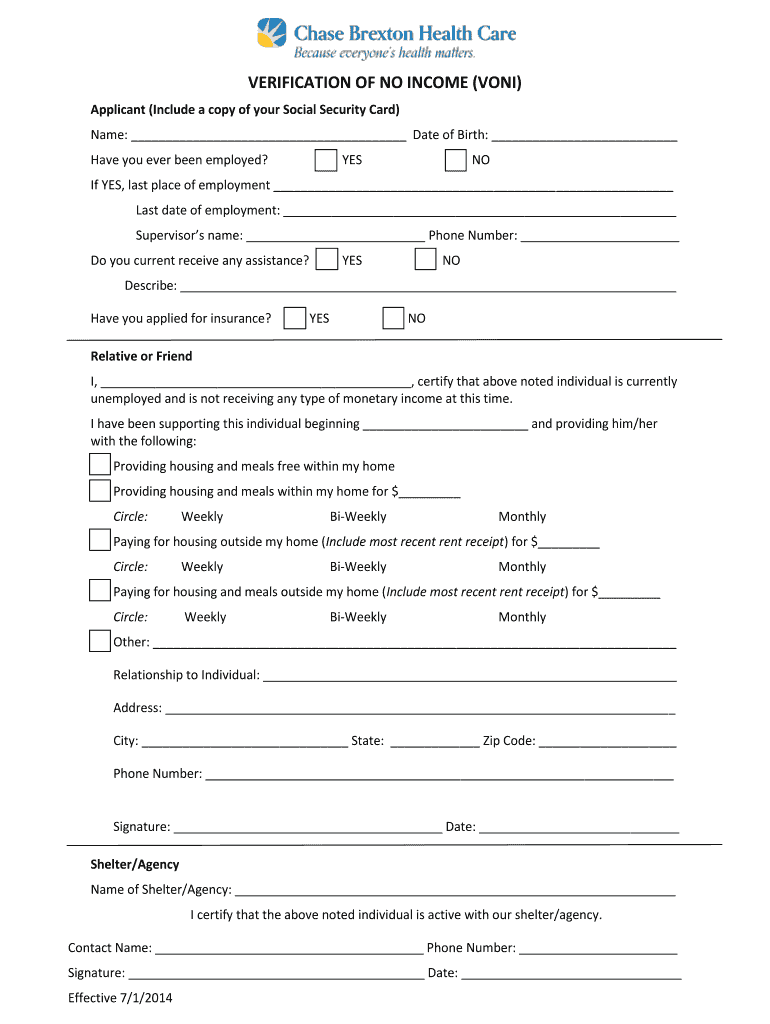
Any person who intentionally fails to give accurate information may be subject to prosecution for fraud. This form is required for income verification if you do not have tax forms available. Agency request the above named individual has applied for assistance from the state of florida. § 435,910, el departamento está solicitando proporcionarle el número de seguro social (ssn), pero.
Hr Employment Verification Questions MEPLOYM
Verification of dependent care expenses. Some forms require adobe acrobat. Agency request the above named individual has applied for assistance from the state of florida. Any person who intentionally fails to give accurate information may be subject to prosecution for fraud. Web de conformidad con el 42 c.f.r.

Verification Of Employment Loss Of Form Substitute teacher
Verification of dependent care expenses. We need specific amounts to determine eligibility. Any person who intentionally fails to give accurate information may be subject to prosecution for fraud. When completing this form please do not use phrases such as “amount varies”, “it varies from month to month”, or “as much as i can”. Web de conformidad con el 42 c.f.r.

How Does Usps Verify Employment PLOYMENT
We need specific amounts to determine eligibility. Please complete each section which has been marked on page 1 and page 2 of this form. Verification of dependent care expenses. Hearings request for public assistance. When completing this form please do not use phrases such as “amount varies”, “it varies from month to month”, or “as much as i can”.

Voe Form with Verification Of Employment Loss Of Form
Web case name _____ case number/cat/seq. Verification of dependent care expenses. When completing this form please do not use phrases such as “amount varies”, “it varies from month to month”, or “as much as i can”. Verification of employment/loss of income. Office address / phone number:

Verification Of Employment Loss Of
Web include details of your business’s income and expenses for the past three months and upload the completed form to your application. Web search florida department of children and families forms by form number, form title, form category, or any combination of these. When completing this form please do not use phrases such as “amount varies”, “it varies from month.

Verification Of Employment Form Employee Forms Craft Employment form
We need specific amounts to determine eligibility. Web search florida department of children and families forms by form number, form title, form category, or any combination of these. Web income verification request to: Please complete each section which has been marked on page 1 and page 2 of this form. Web case name _____ case number/cat/seq.
No Verification Letter Fill Out and Sign Printable PDF
Some forms require adobe acrobat. § 435,910, el departamento está solicitando proporcionarle el número de seguro social (ssn), pero no es necesario que nos proporcione el número de seguro social bajo la ley. Name:_______________________________ ssn:______________________ id number:______________________ s ection i: Verification of employment/loss of income. The following provide links to every form and application that governs the licensing, registration, training.
Verification Of Employment Loss Of Fill Out and Sign Printable
Verification of dependent care expenses. Web case name _____ case number/cat/seq. Web de conformidad con el 42 c.f.r. This form is required for income verification if you do not have tax forms available. § 435,910, el departamento está solicitando proporcionarle el número de seguro social (ssn), pero no es necesario que nos proporcione el número de seguro social bajo la.

Verification form Dcf New Sample In E Verification form 9 Free
Web de conformidad con el 42 c.f.r. Please complete each section which has been marked on page 1 and page 2 of this form. Name:_______________________________ ssn:______________________ id number:______________________ s ection i: Web case name _____ case number/cat/seq. Verification of employment/loss of income.
Case Name:___________________________________________ Case Number:___________________ Month:___________________ For Every Day You Work,.
Any person who intentionally fails to give accurate information may be subject to prosecution for fraud. Please complete each section which has been marked on page 1 and page 2 of this form. This form is required for income verification if you do not have tax forms available. Some forms require adobe acrobat.
Web Search Florida Department Of Children And Families Forms By Form Number, Form Title, Form Category, Or Any Combination Of These.
Web income verification request to: Hearings request for public assistance. Verification of dependent care expenses. Web include details of your business’s income and expenses for the past three months and upload the completed form to your application.
The Following Provide Links To Every Form And Application That Governs The Licensing, Registration, Training And Accreditation Processes Of Child Care Facilities And Homes Within The State Of Florida.
Web case name _____ case number/cat/seq. We need specific amounts to determine eligibility. Web de conformidad con el 42 c.f.r. § 435,910, el departamento está solicitando proporcionarle el número de seguro social (ssn), pero no es necesario que nos proporcione el número de seguro social bajo la ley.
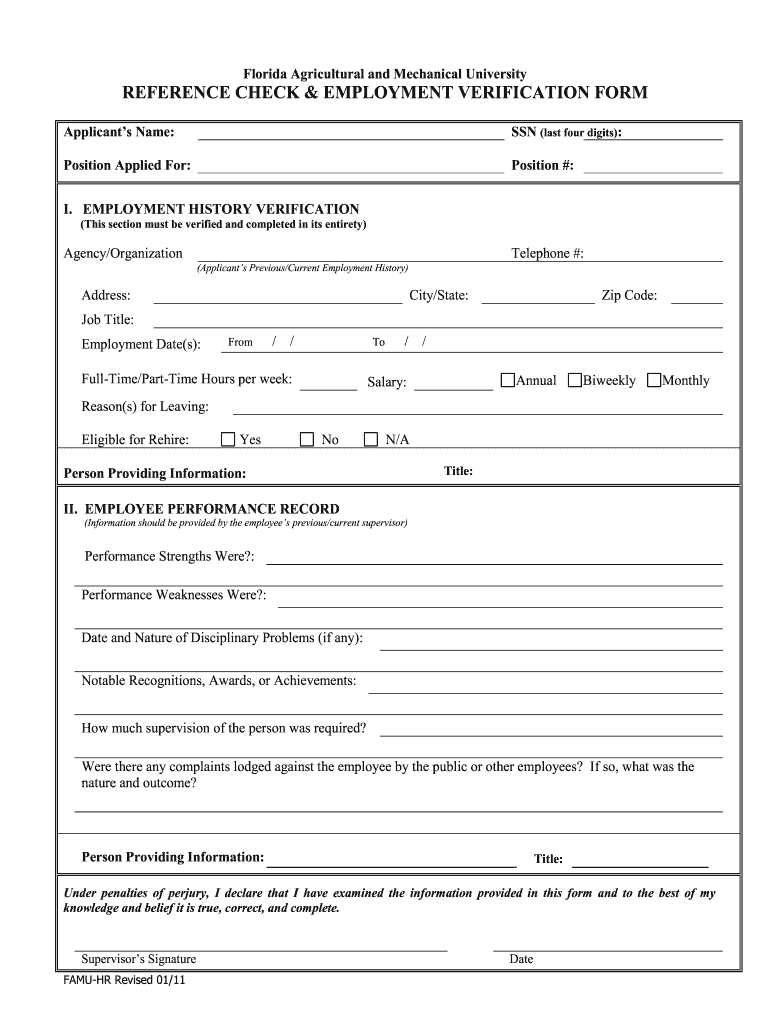
Agency Request The Above Named Individual Has Applied For Assistance From The State Of Florida.
Name:_______________________________ ssn:______________________ id number:______________________ s ection i: Verification of employment/loss of income. Office address / phone number: When completing this form please do not use phrases such as “amount varies”, “it varies from month to month”, or “as much as i can”.