Kaiser Permanente Enrollment Form
Kaiser Permanente Enrollment Form - Web kaiser permanente offers individual health insurance plans for people of all ages. Live in the plan’ s service area important: Web to join a plan, you must: The items in section 2 are optional — you can’t be denied coverage because you don’t fill them out. You must complete all items in section 1. Web forms and publications looking for information about the services we offer? Find a doctor, transfer your prescriptions, and register on kp.org. Web with kaiser permanente, you get a partner in health on top of great care and coverage. Please tell us your location so we can take you to information customized for that area. Medicare part a (hospital insurance) medicare part b (medical insurance) when do i use this form?
Be a united states citizen or be lawfully present in the u.s. You can join a plan: Web to join a plan, you must: Find care our organization member support visit our other sites. Web forms and publications looking for information about the services we offer? California colorado district of columbia georgia hawaii maryland oregon virginia washington View, download, or print commonly used forms, guidebooks, handbooks, and other publications. Web with kaiser permanente, you get a partner in health on top of great care and coverage. Web kaiser permanente offers individual health insurance plans for people of all ages. The items in section 2 are optional — you can’t be denied coverage because you don’t fill them out.
Live in the plan’ s service area important: View, download, or print commonly used forms, guidebooks, handbooks, and other publications. Web kaiser permanente offers individual health insurance plans for people of all ages. Web forms and publications looking for information about the services we offer? Apply now for an individual and family plan that’s right for you. Medicare part a (hospital insurance) medicare part b (medical insurance) when do i use this form? Enrollment/change reason employee family employee/applicant signature and date your agency does not need to complete the section titled “to be completed by employer” Web with kaiser permanente, you get a partner in health on top of great care and coverage. Web if you’re new to kaiser permanente, we’ll help you get set up. Find care our organization member support visit our other sites.

Kaiser Permanente Hawaii Federal Open Enrollment Video YouTube
Apply now for an individual and family plan that’s right for you. View, download, or print commonly used forms, guidebooks, handbooks, and other publications. The items in section 2 are optional — you can’t be denied coverage because you don’t fill them out. Be a united states citizen or be lawfully present in the u.s. Find care our organization member.

20202022 Kaiser Permanente Employee Enrollment and Change Form Fill
The items in section 2 are optional — you can’t be denied coverage because you don’t fill them out. Web with kaiser permanente, you get a partner in health on top of great care and coverage. Find a doctor, transfer your prescriptions, and register on kp.org. Please tell us your location so we can take you to information customized for.

Kaiser Permanente Individual Family Plan Disenrollment Request Form
Web small business employee enrollment use this form to enroll in kaiser permanente. Web what do i need to complete this form? Enrollment/change reason employee family employee/applicant signature and date your agency does not need to complete the section titled “to be completed by employer” Web with kaiser permanente, you get a partner in health on top of great care.
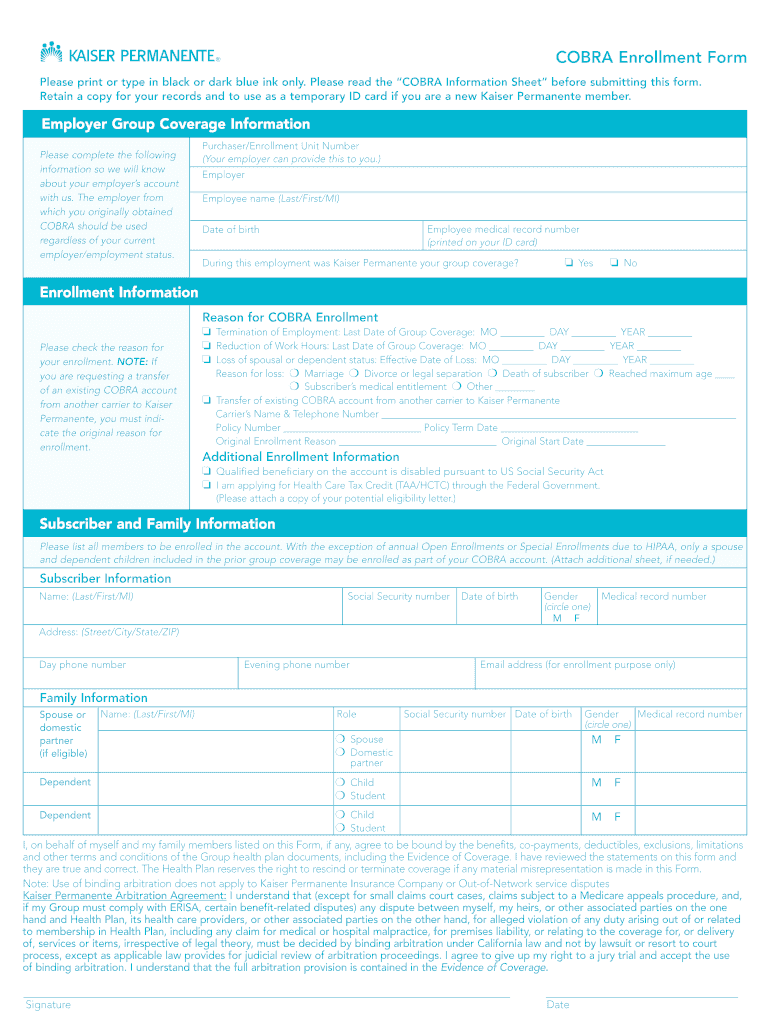
Kaiser Permanente COBRA Enrollment Form (PDF) MEBA mymeba Fill
Live in the plan’ s service area important: You must complete all items in section 1. Find a doctor, transfer your prescriptions, and register on kp.org. Web with kaiser permanente, you get a partner in health on top of great care and coverage. Web kaiser permanente offers individual health insurance plans for people of all ages.

CA Kaiser Permanente 343169123B 20192022 Fill and Sign Printable
Return the signed form to: You can join a plan: Kaiser permanente medicare unit p.o. To join a medicare advantage plan, you must also have both: Web with kaiser permanente, you get a partner in health on top of great care and coverage.

Kaiser Enrollment Form Enrollment Form
You can join a plan: Web kaiser permanente offers individual health insurance plans for people of all ages. Web small business employee enrollment use this form to enroll in kaiser permanente. Live in the plan’ s service area important: Find care our organization member support visit our other sites.

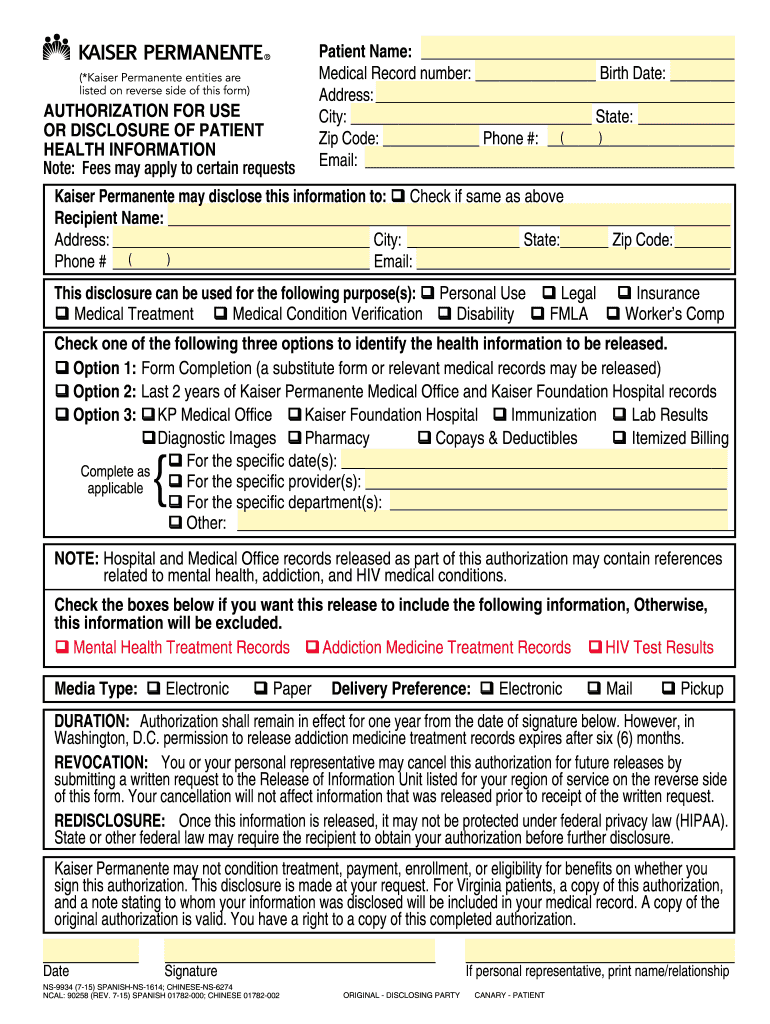
Kaiser Permanente Form For Patient Health Onfo Fill Online, Printable
California colorado district of columbia georgia hawaii maryland oregon virginia washington View, download, or print commonly used forms, guidebooks, handbooks, and other publications. The items in section 2 are optional — you can’t be denied coverage because you don’t fill them out. Find a doctor, transfer your prescriptions, and register on kp.org. You must complete all items in section 1.
Kaiser Permanente Forms Medical Release Forms Fill Out and Sign
Web small business employee enrollment use this form to enroll in kaiser permanente. Learn more about our plans and how to enroll yourself or your family. You must complete all items in section 1. Web what do i need to complete this form? Kaiser permanente medicare unit p.o.

Kaiser Senior Advantage Plus Disenrollment Form Form Resume
Web kaiser permanente offers individual health insurance plans for people of all ages. Web small business employee enrollment use this form to enroll in kaiser permanente. The items in section 2 are optional — you can’t be denied coverage because you don’t fill them out. Find care our organization member support visit our other sites. Web to join a plan,.
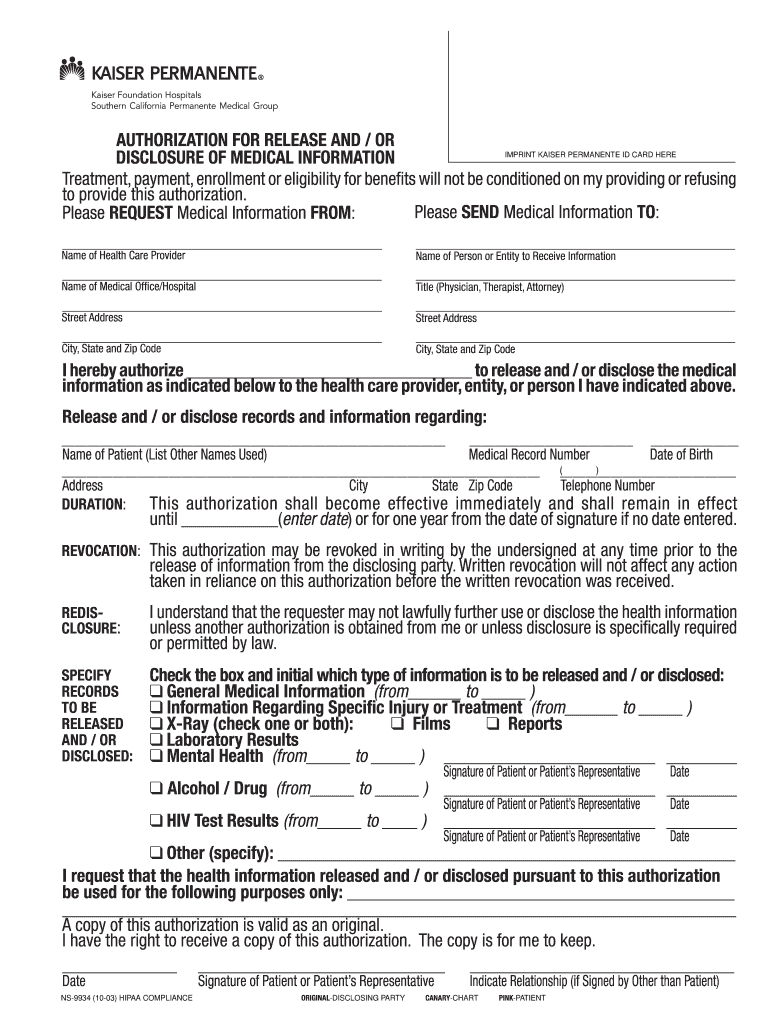
Kaiser permanente form ns 9934 Fill out & sign online DocHub
Web how to complete and submit this form complete the following sections: Return the signed form to: Please tell us your location so we can take you to information customized for that area. Enrollment/change reason employee family employee/applicant signature and date your agency does not need to complete the section titled “to be completed by employer” •our medicare number (the.
Web If You’re New To Kaiser Permanente, We’ll Help You Get Set Up.
Web small business employee enrollment use this form to enroll in kaiser permanente. Kaiser permanente medicare unit p.o. California colorado district of columbia georgia hawaii maryland oregon virginia washington Be a united states citizen or be lawfully present in the u.s.
Learn More About Our Plans And How To Enroll Yourself Or Your Family.
You must complete all items in section 1. You can join a plan: View, download, or print commonly used forms, guidebooks, handbooks, and other publications. Web with kaiser permanente, you get a partner in health on top of great care and coverage.
Web How To Complete And Submit This Form Complete The Following Sections:
Web kaiser permanente offers individual health insurance plans for people of all ages. To join a medicare advantage plan, you must also have both: Web to join a plan, you must: Find a doctor, transfer your prescriptions, and register on kp.org.
Web What Do I Need To Complete This Form?
Return the signed form to: Enrollment/change reason employee family employee/applicant signature and date your agency does not need to complete the section titled “to be completed by employer” The items in section 2 are optional — you can’t be denied coverage because you don’t fill them out. Medicare part a (hospital insurance) medicare part b (medical insurance) when do i use this form?