Medicaid Referral Form
Medicaid Referral Form - Web program and the referral is not a guarantee of payment. Web referral forms in many cases, a referral to another doctor or clinic is needed for services or care. Request for information or action: Now, creating a medicaid referral form takes not more than 5 minutes. Web email completed application to apply@medicaid.alabama.gov. For services scheduled in advance, submit fax to Department of health and human services. Web physician first and last name medicaid provider id# date of referral i have performed a clinical assessment of the patient named above whom i am referring for the service listed. Programs and services applying for medicaid provider billing manuals integrated care networks link to: Web medicaid prior authorization forms.
Web follow the simple instructions below: The centers for medicare & medicaid services (cms) is a federal agency within the u.s. Request for information or action: Department of health and human services. Keep a duplicate copy for your records in the member’s medical chart. Web supplemental security income referral h1019: Now, creating a medicaid referral form takes not more than 5 minutes. Web email completed application to apply@medicaid.alabama.gov. Web referral forms in many cases, a referral to another doctor or clinic is needed for services or care. Web medicaid prior authorization forms.
Keep a duplicate copy for your records in the member’s medical chart. Web program and the referral is not a guarantee of payment. Web physician first and last name medicaid provider id# date of referral i have performed a clinical assessment of the patient named above whom i am referring for the service listed. Complete and mail/fax the original copy of the form to the provider to whom you are referring. Web email completed application to apply@medicaid.alabama.gov. Web medicaid prior authorization forms. Web referral forms in many cases, a referral to another doctor or clinic is needed for services or care. Save or instantly send your ready documents. Web follow the simple instructions below: For services scheduled in advance, submit fax to

Texas Referral Authorization Form Pdf Fill Out and Sign Printable PDF
Web complete medicaid referral form online with us legal forms. Save or instantly send your ready documents. Web email completed application to apply@medicaid.alabama.gov. Complete and mail/fax the original copy of the form to the provider to whom you are referring. Web physician first and last name medicaid provider id# date of referral i have performed a clinical assessment of the.
Application For Nebraska Medicaid For Aged And Disabled Dhhs Ne
The centers for medicare & medicaid services (cms) is a federal agency within the u.s. Keep a duplicate copy for your records in the member’s medical chart. Web referral forms in many cases, a referral to another doctor or clinic is needed for services or care. Save or instantly send your ready documents. However, with our predesigned online templates, everything.
Specialty Care Referral Form Delta Dental Utah Medicaid Dental
Web medicaid prior authorization forms. Web supplemental security income referral h1019: The centers for medicare & medicaid services (cms) is a federal agency within the u.s. Web complete medicaid referral form online with us legal forms. Web physician first and last name medicaid provider id# date of referral i have performed a clinical assessment of the patient named above whom.
DMS320 Arkansas Medicaid
Web follow the simple instructions below: Easily fill out pdf blank, edit, and sign them. Web supplemental security income referral h1019: Web email completed application to apply@medicaid.alabama.gov. Keep a duplicate copy for your records in the member’s medical chart.
![50 Referral Form Templates [Medical & General] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2019/02/referral-form-template-38-790x1022.jpg)
50 Referral Form Templates [Medical & General] ᐅ TemplateLab
Easily fill out pdf blank, edit, and sign them. Save or instantly send your ready documents. Now, creating a medicaid referral form takes not more than 5 minutes. Web authorization/referral request form please complete all fields on this form and be sure to include an area code along with your telephone and fax numbers. Complete and mail/fax the original copy.
Physician Referral Form Center For Speech & Language printable pdf
Complete and mail/fax the original copy of the form to the provider to whom you are referring. Request for information or action: The centers for medicare & medicaid services (cms) is a federal agency within the u.s. Keep a duplicate copy for your records in the member’s medical chart. Web complete medicaid referral form online with us legal forms.
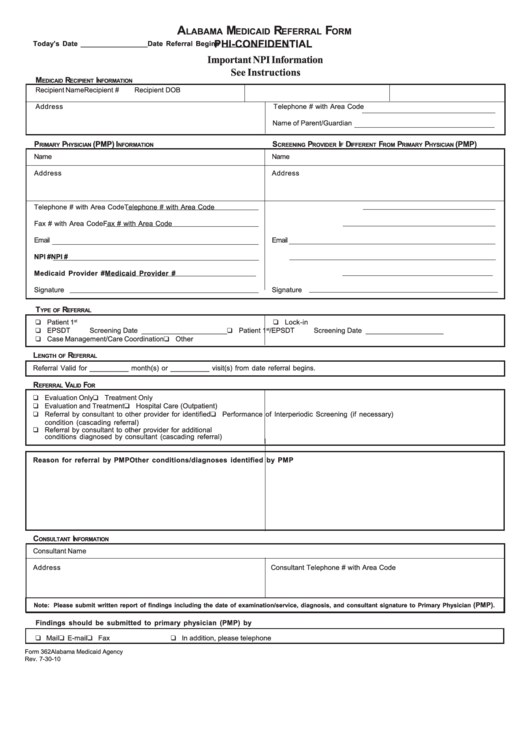
Fillable Form 362 Alabama Medicaid Referral Form printable pdf download
Many cms program related forms are available in portable document format (pdf). Web program and the referral is not a guarantee of payment. Complete and mail/fax the original copy of the form to the provider to whom you are referring. Save or instantly send your ready documents. Web email completed application to apply@medicaid.alabama.gov.
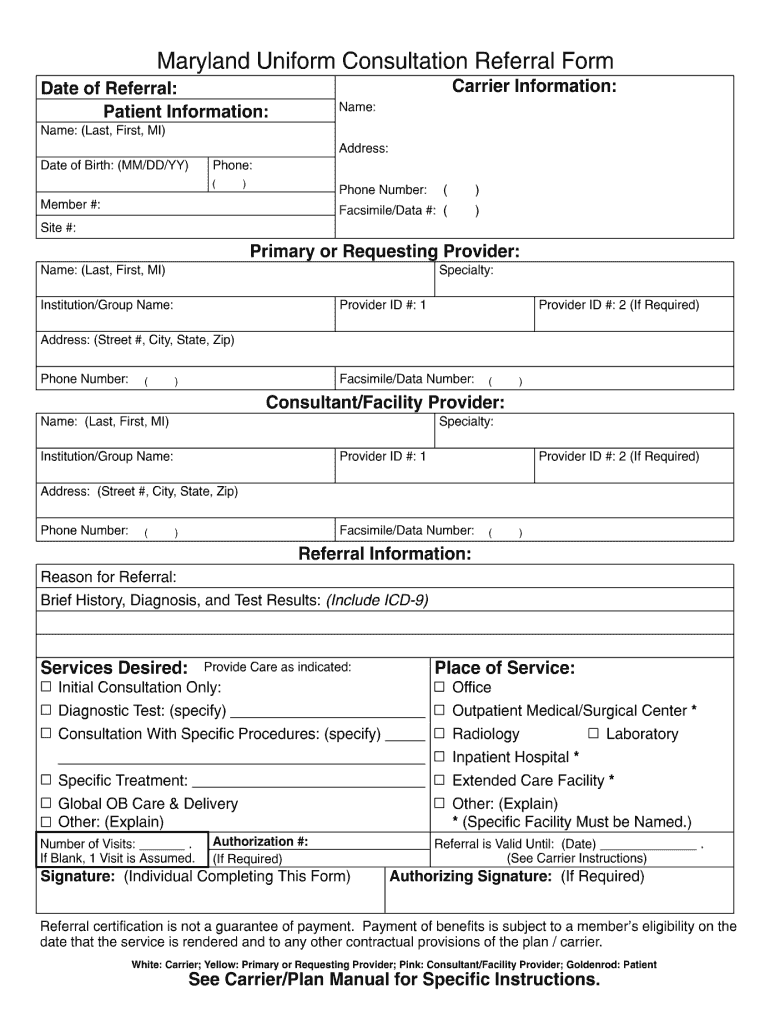
Maryland Uniform Fill Online, Printable, Fillable, Blank pdfFiller
Web supplemental security income referral h1019: Programs and services applying for medicaid provider billing manuals integrated care networks link to: Web complete medicaid referral form online with us legal forms. For services scheduled in advance, submit fax to Now, creating a medicaid referral form takes not more than 5 minutes.

fegs nassau county health home referral form Medicaid Psychiatry
For services scheduled in advance, submit fax to Web referral forms in many cases, a referral to another doctor or clinic is needed for services or care. Web physician first and last name medicaid provider id# date of referral i have performed a clinical assessment of the patient named above whom i am referring for the service listed. Web authorization/referral.
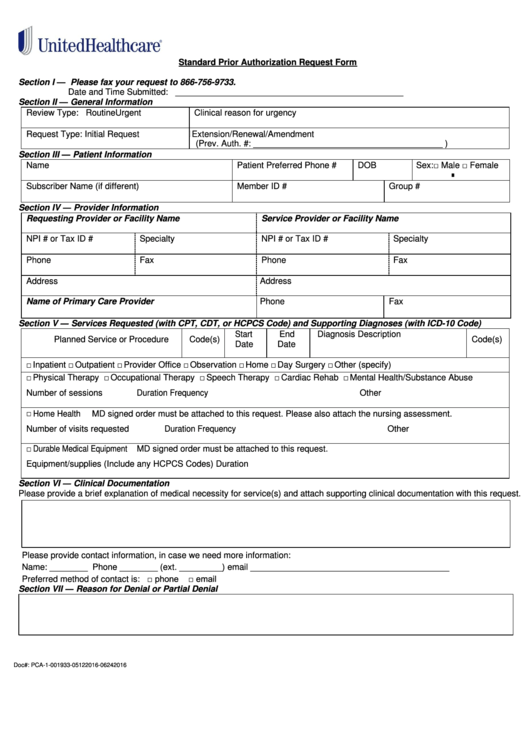
Fillable Standard Prior Authorization Request Form United Healthcare
Web complete medicaid referral form online with us legal forms. Save or instantly send your ready documents. For services scheduled in advance, submit fax to Web program and the referral is not a guarantee of payment. The centers for medicare & medicaid services (cms) is a federal agency within the u.s.
Web Authorization/Referral Request Form Please Complete All Fields On This Form And Be Sure To Include An Area Code Along With Your Telephone And Fax Numbers.
Web referral forms in many cases, a referral to another doctor or clinic is needed for services or care. Easily fill out pdf blank, edit, and sign them. For services scheduled in advance, submit fax to The centers for medicare & medicaid services (cms) is a federal agency within the u.s.
Many Cms Program Related Forms Are Available In Portable Document Format (Pdf).
Web medicaid prior authorization forms. Save or instantly send your ready documents. However, with our predesigned online templates, everything gets simpler. Web supplemental security income referral h1019:
Web Complete Medicaid Referral Form Online With Us Legal Forms.
Keep a duplicate copy for your records in the member’s medical chart. Now, creating a medicaid referral form takes not more than 5 minutes. Web follow the simple instructions below: Department of health and human services.
Request For Information Or Action:
Programs and services applying for medicaid provider billing manuals integrated care networks link to: Complete and mail/fax the original copy of the form to the provider to whom you are referring. Web email completed application to apply@medicaid.alabama.gov. Web physician first and last name medicaid provider id# date of referral i have performed a clinical assessment of the patient named above whom i am referring for the service listed.