Medicaid Wheelchair Form
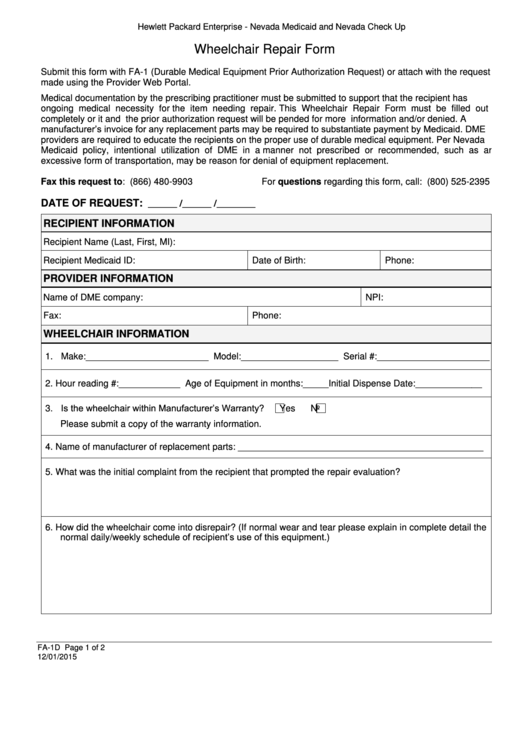
Medicaid Wheelchair Form - Web the intent of this form is to secure sufficient information to determine the medical necessity for a custom wheelchair request submitted for prior approval to florida medicaid. This form must be completed by the licensed therapist or the. Which doctors and drugstores you can use. Preceding this order, and i am enrolled with georgia medicaid for the purpose of ordering, referring, or prescribing medical. However, coverage varies from state to state. Hard copy forms may be available from intermediaries, carriers, state agencies, local social security offices or end stage. Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s. Web contact a local cap/da case management entity in the county of residence of the applicant to request a cap/da referral. It must be completed by an alabama licensed physical therapist (pt)/occupational therapist (ot). You have a health condition that causes significant dificulty moving around in your home
You have a health condition that causes significant dificulty moving around in your home Nc medicaid contact center phone: This form is a required attachment to the alabama medicaid prior review andauthorization form (form 342). Web this form should be completed by a healthcare professional who is aware and participating in the care of the member and who can provide information on the appropriate level of transportation that the individual needs. Forms for durable medical equipment, orthotics and prosthetics. Web allow at least 60 days for medicare to receive and process your claim request. Web revised 1/1/2019 cmn for manual wheelchair page 1of 2. It must be completed by an alabama licensed physical therapist (pt)/occupational therapist (ot). With pa on the portal, documents will be immediately received by the pa department, resulting in a quicker decision. (order form) healthchek & pregnancy related services information sheet.
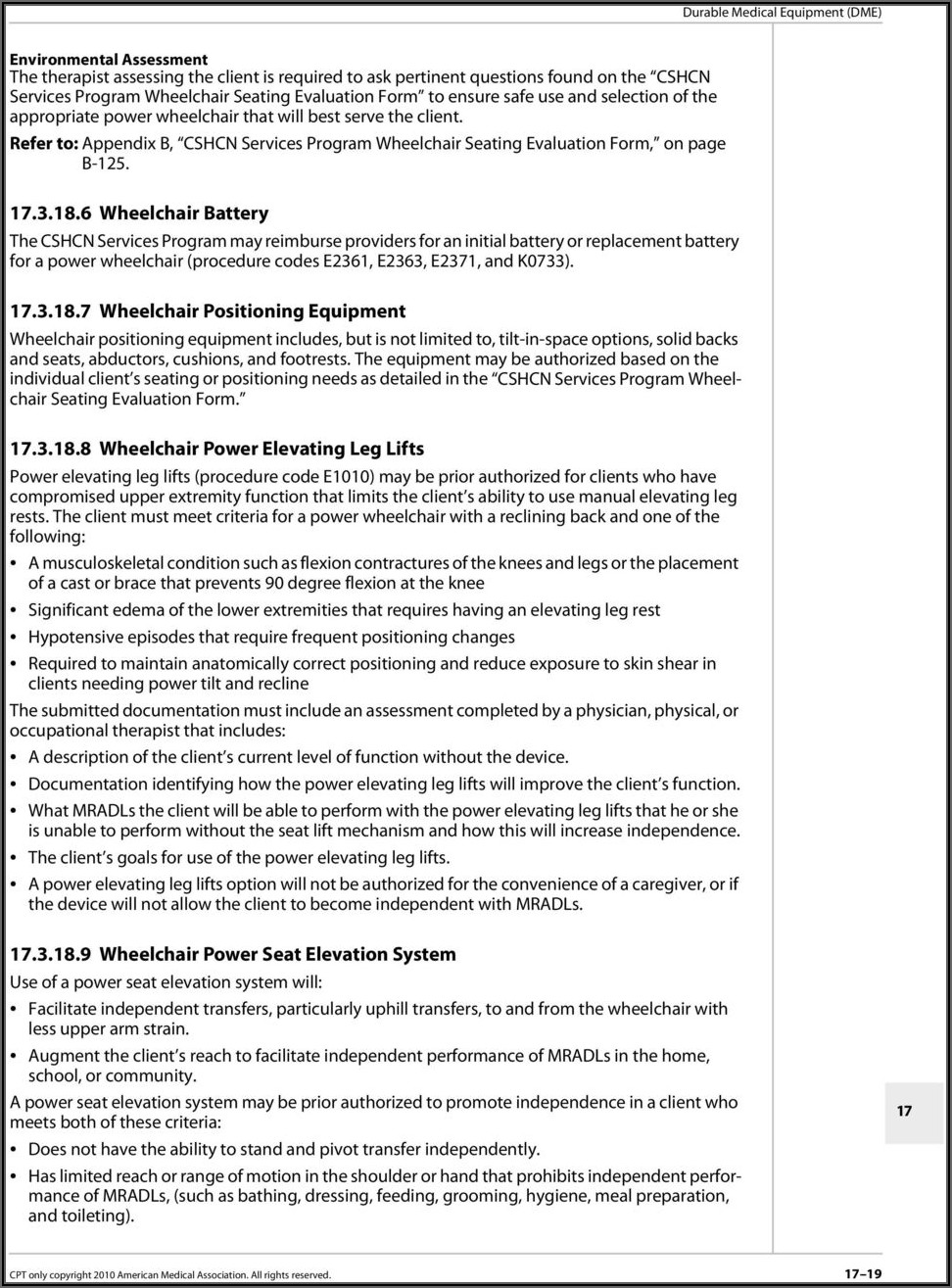
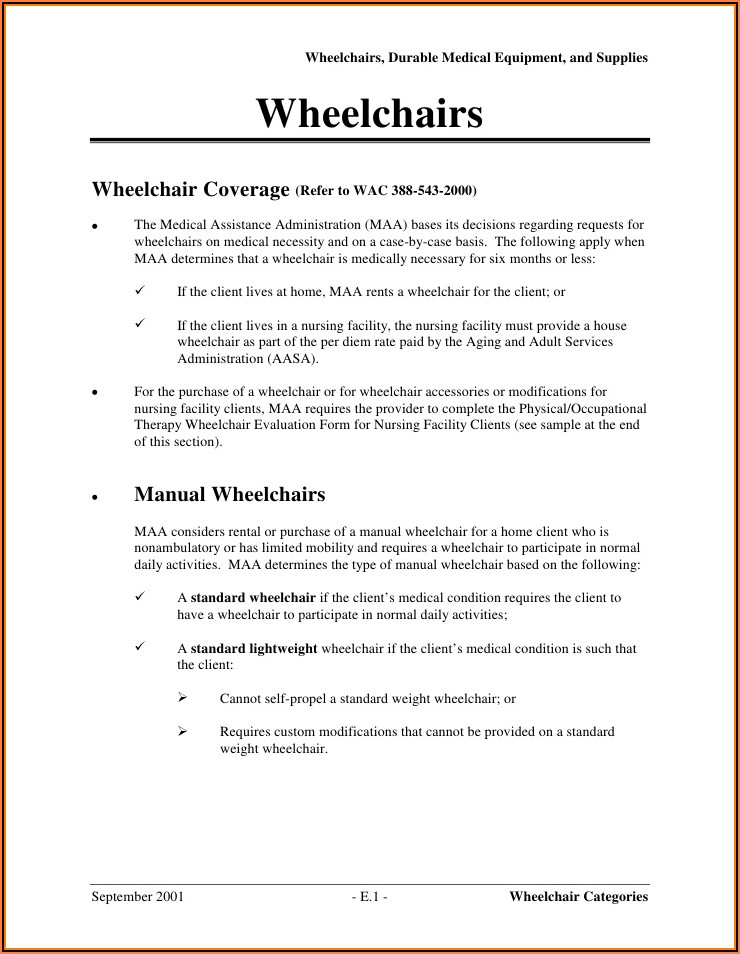
Nc medicaid contact center phone: Power wheelchairs can be covered as dme under medicaid; Web the doctor treating your condition submits a written order stating that you have a medical need for a wheelchair or scooter for use in your home. Board and exit the vehicle unassisted, or is a collapsible wheelchair user who can approach the vehicle and transfer without assistance, but cannot utilize public transportation. Department of health and human services. Web wheelchair/scooter/stroller seating assessment form (ccp/home health services) (8 pages) submit your prior authorization using tmhp’s pa on the portal and receive request decisions more quickly than faxed requests. You have limited mobility and meet all of these conditions: (order form) application for health coverage & help paying costs. Hard copy forms may be available from intermediaries, carriers, state agencies, local social security offices or end stage. Don’t let anyone else use your medicaid card.
Medicaid Wheelchair Evaluation Form Form Resume Examples GM9Ooog09D
Hard copy forms may be available from intermediaries, carriers, state agencies, local social security offices or end stage. Mental health and substance use targeted case management, certificates of need, individual service needs and discharge planning. Web the intent of this form is to secure sufficient information to determine the medical necessity for a custom wheelchair request submitted for prior approval.
Medicare Wheelchair Face To Face Form Form Resume Examples A19XjQdV4k
Click here to enter text. Web contact a local cap/da case management entity in the county of residence of the applicant to request a cap/da referral. This form is a required attachment to the alabama medicaid prior review andauthorization form (form 342). Web mobility assessment and prior authorization (pa) request. With pa on the portal, documents will be immediately received.
93 Medicaid Forms And Templates free to download in PDF
Web contact a local cap/da case management entity in the county of residence of the applicant to request a cap/da referral. Mental health and substance use targeted case management, certificates of need, individual service needs and discharge planning. Web the intent of this form is to secure sufficient information to determine the medical necessity for a custom wheelchair request submitted.

Medicare Wheelchair Face To Face Form Form Resume Examples YL5zmbyDzV
(order form) healthchek & pregnancy related services information sheet. This form is a required attachment to the alabama medicaid prior review andauthorization form (form 342). It must be completed by an alabama licensed physical therapist (pt)/occupational therapist (ot). Web medicaid will only pay for a motorized wheelchair if the individual has a medical need for the specific type of electric.

How Often Will Medicaid Pay for a Wheelchair? Wheelchair Junkie
Board and exit the vehicle unassisted, or is a collapsible wheelchair user who can approach the vehicle and transfer without assistance, but cannot utilize public transportation. Sterilization consent form (spanish) urine drug screen information form. (order form) application for health coverage & help paying costs. Don’t let anyone else use your medicaid card. Web medicaid will only pay for a.
Medicare Wheelchair Assessment Form Form Resume Examples VX5JKzROjv
Stamps are not an acceptable form of authentication for the date or signature on a certificate of medical Plan, serve and document quality of care for individuals residing in adult care homes. (order form) healthchek & pregnancy related services information sheet. As a reminder to providers, when requesting authorization for a power wheelchair, a “wheelchair training checklist form” must be.
Mississippi Medicaid Wheelchair Evaluation Form Form Resume
Web medicaid will only pay for a motorized wheelchair if the individual has a medical need for the specific type of electric wheelchair he or she needs. With pa on the portal, documents will be immediately received by the pa department, resulting in a quicker decision. There must also be a doctor’s prescription. Hard copy forms may be available from.
Florida Medicaid Wheelchair Evaluation Form Form Resume Examples
Print your name shown on your medicare card (last name, first name, middle name). This form is a required attachment to the alabama medicaid prior review andauthorization form (form 342). ☐ yes ☐ no if yes, explain: Web only applicable sections of this form need to be completed and. Power wheelchairs can be covered as dme under medicaid;
Medicare Manual Wheelchair Evaluation Form Form Resume Examples
You have limited mobility and meet all of these conditions: Web allow at least 60 days for medicare to receive and process your claim request. Web is the mobility limitation secondary to severe neurological condition, myopathy, or congenital skeletal deformity? Preceding this order, and i am enrolled with georgia medicaid for the purpose of ordering, referring, or prescribing medical. Board.
Ohio Medicaid Wheelchair Evaluation Form Form Resume Examples
Web mobility assessment and prior authorization (pa) request. Web revised 1/1/2019 cmn for manual wheelchair page 1of 2. Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s. Web is the mobility limitation secondary to severe neurological condition, myopathy, or congenital skeletal deformity? Web the doctor treating your condition submits a written order stating.
As A Reminder To Providers, When Requesting Authorization For A Power Wheelchair, A “Wheelchair Training Checklist Form” Must Be Completed.
Web only applicable sections of this form need to be completed and. Sterilization consent form (spanish) urine drug screen information form. It must be completed by an alabama licensed physical therapist (pt)/occupational therapist (ot). Department of health and human services.
Alabama Medicaid Will Only Reimburse For The Physical Therapy
Which doctors and drugstores you can use. Print your name shown on your medicare card (last name, first name, middle name). Web the intent of this form is to secure sufficient information to determine the medical necessity for a custom wheelchair request submitted for prior approval to florida medicaid. Click here to enter text.
Web Revised 1/1/2019 Cmn For Manual Wheelchair Page 1Of 2.
Web wheelchair/scooter/stroller seating assessment form (ccp/home health services) (8 pages) submit your prior authorization using tmhp’s pa on the portal and receive request decisions more quickly than faxed requests. Web take the your texas medicaid card to doctor visits and to the drugstore. You have a health condition that causes significant dificulty moving around in your home Nc medicaid contact center phone:
Upload This Request Through The Provider Web Portal.
Web allow at least 60 days for medicare to receive and process your claim request. The centers for medicare & medicaid services (cms) has developed a certificate of medical necessity (cmn) form for motorized wheelchairs (form hcfa 843) and povs (form hcfa 850). Board and exit the vehicle unassisted, or is a collapsible wheelchair user who can approach the vehicle and transfer without assistance, but cannot utilize public transportation. Stamps are not an acceptable form of authentication for the date or signature on a certificate of medical