Medical Clearance Form For Dental Extraction
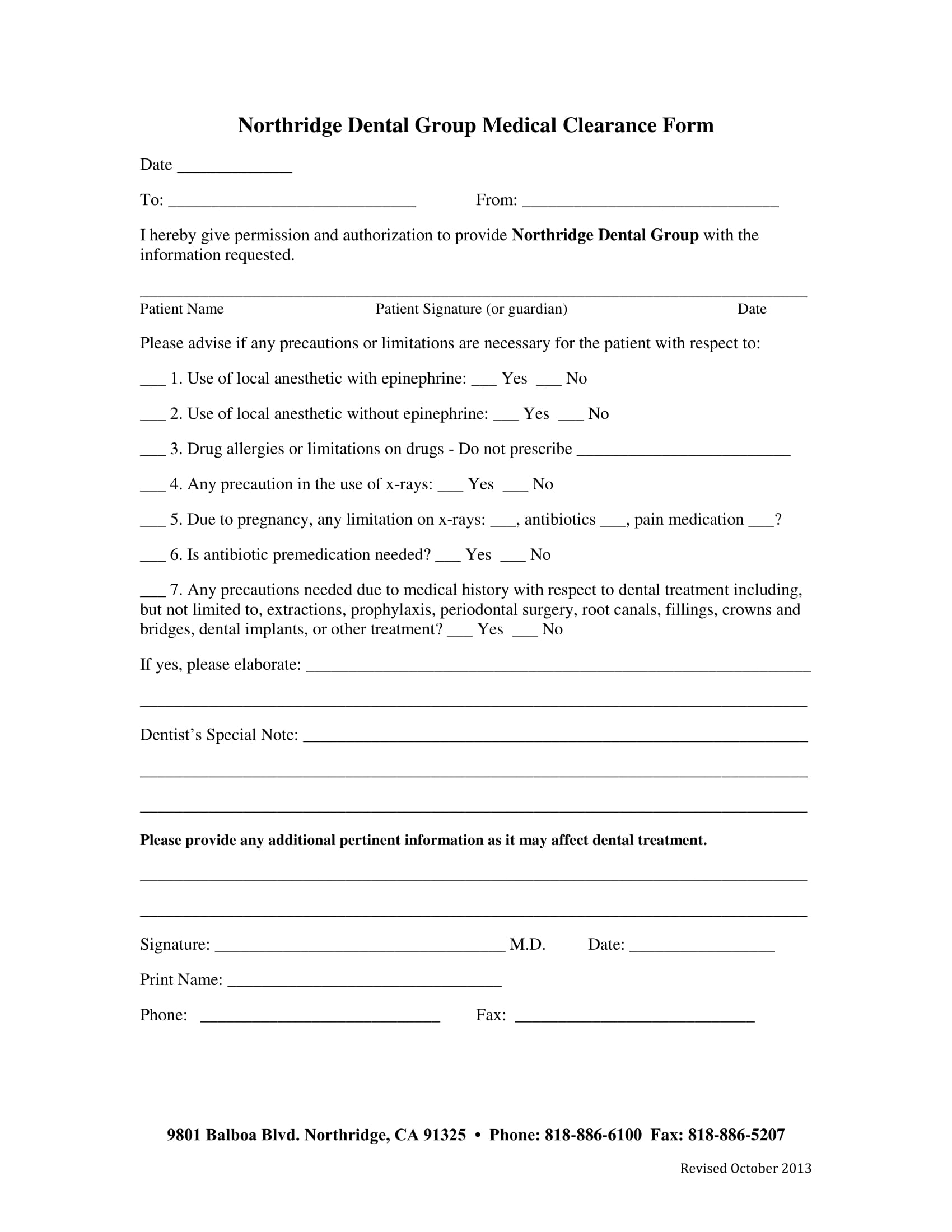
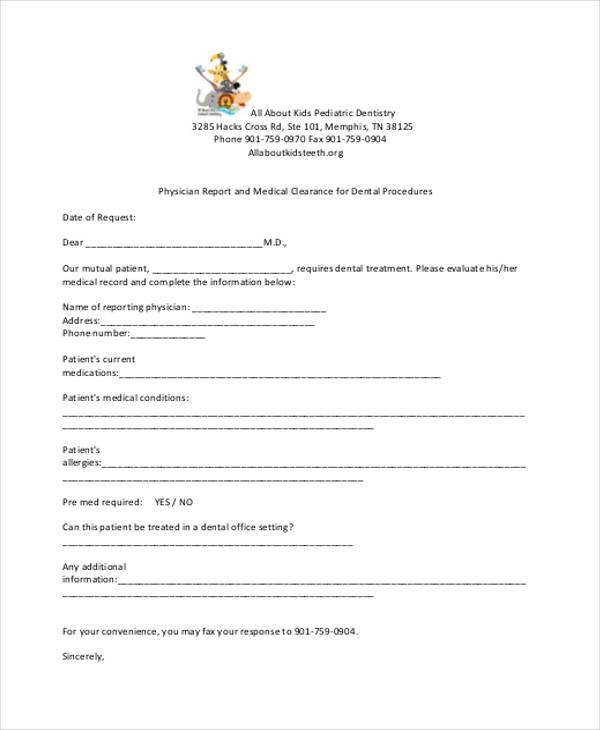
Medical Clearance Form For Dental Extraction - Web request for medical clearance request for medical clearance patient name dear the above name patient has indicated that you are his/her physician. Easily fill out pdf blank, edit, and sign them. Web medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical. Web to proceed with dental treatment, this form is required from a medical physician. Web the physician will assess the risk of dental surgery based on the patient past and current condition in four categories: Huntington beach, ca 92646 o. Web are you thinking about getting medical clearance form for dental to fill? Web the forms in this library are intended to be adapted for the organization's specific needs. Our dentists are devoted to providing kansas city with expert dental care. Web medical clearance form (219)663 advanced dental concepts 10780 randolph street crown point, in 46307.
Web medical clearance for dental treatment. Easily fill out pdf blank, edit, and sign them. Web dental clearance letter re _____ dob_____ mrn_____ to whom it may concern: Web the cost for tooth extraction varies widely depending on whether the tooth is impacted. Web medical clearance form (219)663 advanced dental concepts 10780 randolph street crown point, in 46307. Asa i normal healthy patient. Cocodoc is the best platform for you to go, offering you a great and easy to edit version of medical. Ad our friendly team provides comprehensive family dentistry. Web if you’re a dental office manager, use a free dental clearance form template to collect patient information online! Web the forms in this library are intended to be adapted for the organization's specific needs.
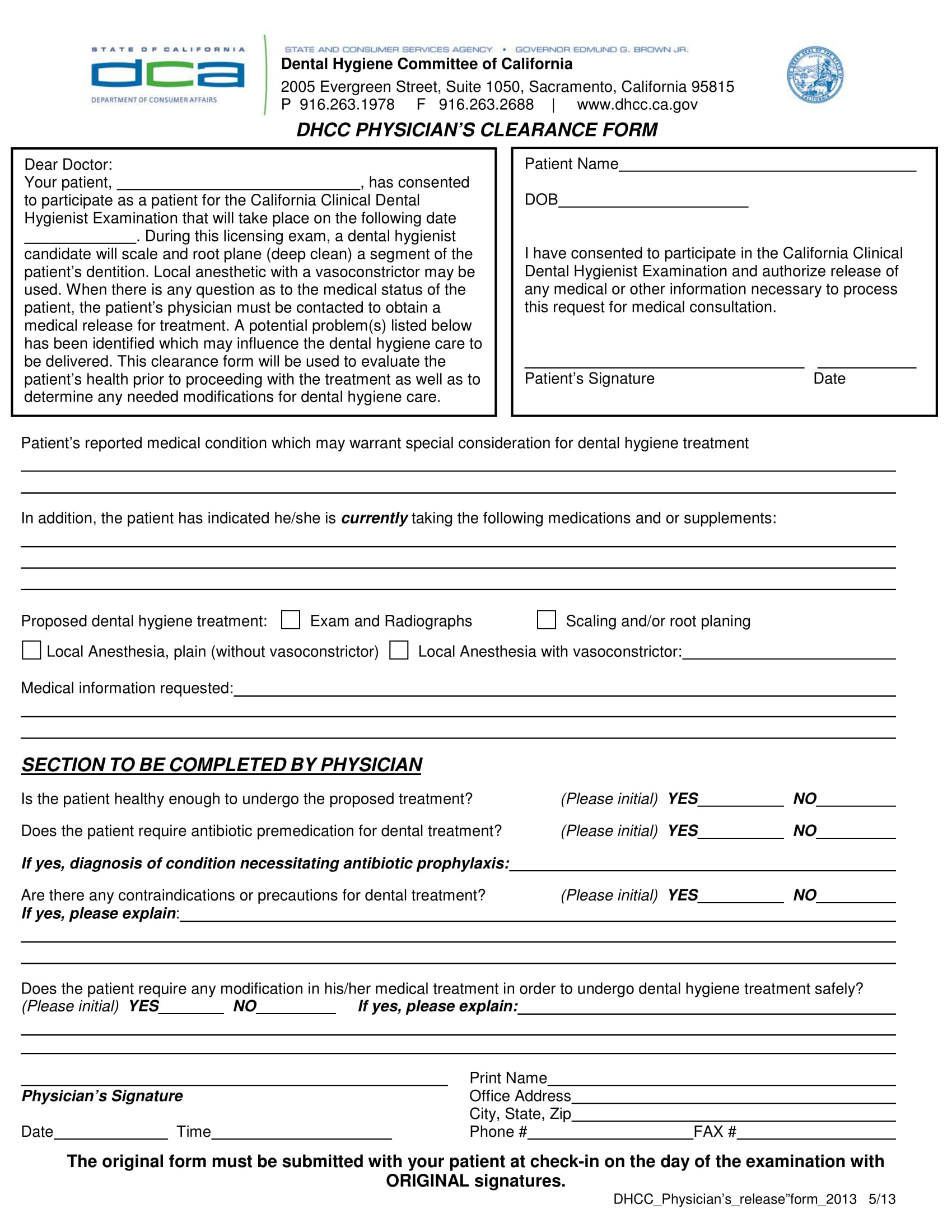
Web the physician will assess the risk of dental surgery based on the patient past and current condition in four categories: Web dental clearance letter re _____ dob_____ mrn_____ to whom it may concern: Web the cost for tooth extraction varies widely depending on whether the tooth is impacted. Save or instantly send your. Cocodoc is the best platform for you to go, offering you a great and easy to edit version of medical. Our dentists are devoted to providing kansas city with expert dental care. Online with us legal forms. Web medical clearance for dental treatment date: Browse the forms in five different categories: Our mutual patient, as noted above, is scheduled for dental treatment at our office.
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Web dental clearance letter re _____ dob_____ mrn_____ to whom it may concern: Huntington beach, ca 92646 o. Cocodoc is the best platform for you to go, offering you a great and easy to edit version of medical. Web if you’re a dental office manager, use a free dental clearance form template to collect patient information online! Web the forms.
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Online with us legal forms. Our dentists are devoted to providing kansas city with expert dental care. Our mutual patient noted above is scheduled to undergo total joint replacement surgery. Browse the forms in five different categories: Web dental clearance letter re _____ dob_____ mrn_____ to whom it may concern:
FREE 30+ Medical Clearance Form Samples in PDF MS Word
Web medical clearance for dental treatment. Online with us legal forms. Web to proceed with dental treatment, this form is required from a medical physician. Web medical clearance form (219)663 advanced dental concepts 10780 randolph street crown point, in 46307. Web the physician will assess the risk of dental surgery based on the patient past and current condition in four.
Printable Medical Clearance Form For Dental Treatment Fill Online
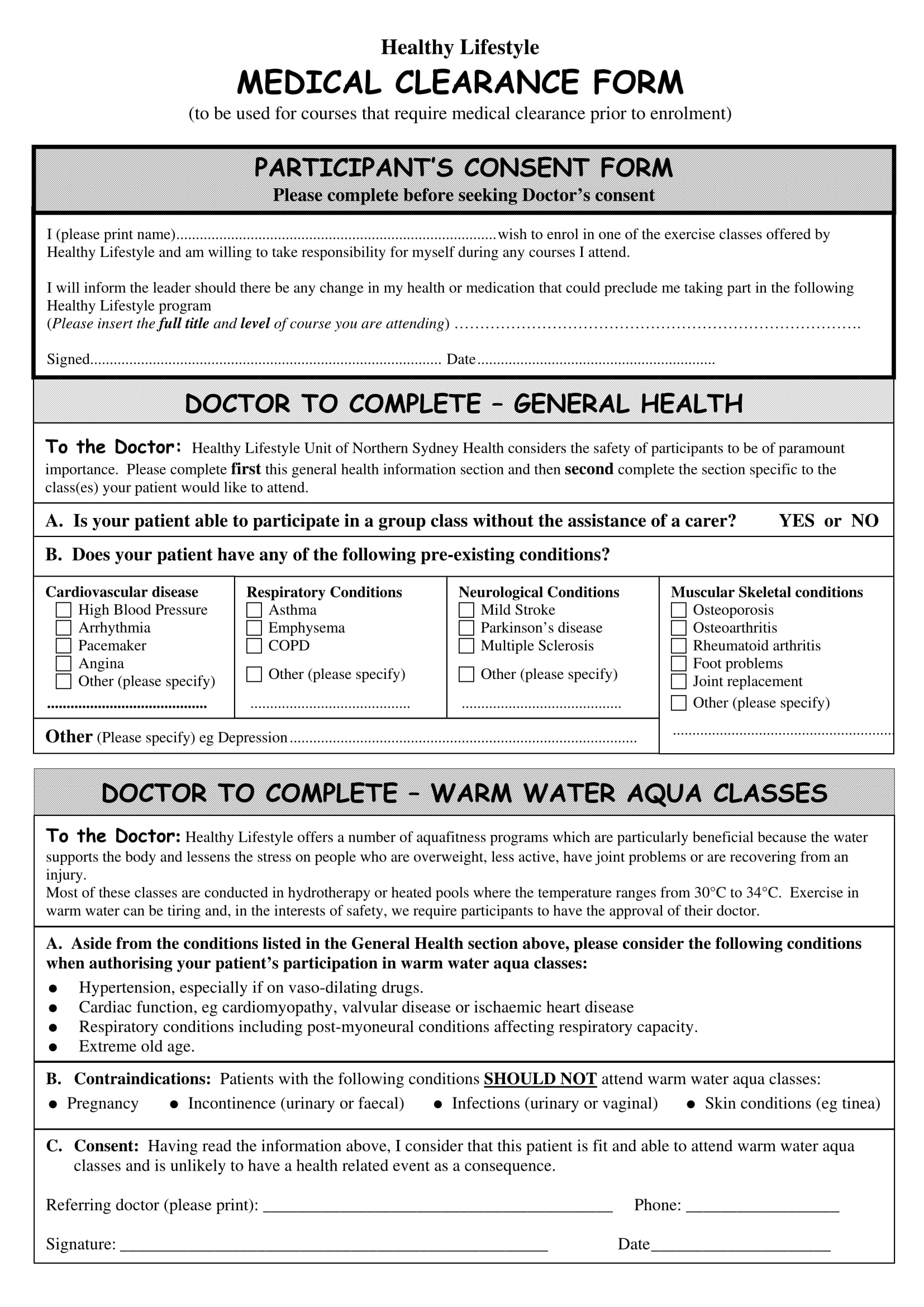
Cocodoc is the best platform for you to go, offering you a great and easy to edit version of medical. Web this article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental procedures, such as cleanings,. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in.
Surgery Medical Clearance Form Fill Out and Sign Printable PDF
Just customize the form to match your dental office’s look. Huntington beach, ca 92646 o. Try a free nexhealth™ demo. Web dental clearance letter re _____ dob_____ mrn_____ to whom it may concern: Web the cost for tooth extraction varies widely depending on whether the tooth is impacted.
Medical Consult Form For Dental Office Medical Art
Online with us legal forms. Ad the dental intake forms system that integrates with your pms. Browse the forms in five different categories: Web are you thinking about getting medical clearance form for dental to fill? This form will include information about patient’s treatment procedures like simple or deep.
Printable Medical Clearance Form For Dental Treatment Printable Word
Our mutual patient noted above is scheduled to undergo total joint replacement surgery. Browse the forms in five different categories: Ad the dental intake forms system that integrates with your pms. Huntington beach, ca 92646 o. Online with us legal forms.
FREE 30+ Sample Medical Clearance Forms in PDF MS Word
Learn more about digitizing your dental intake forms with nexhealth™. Asa i normal healthy patient. Try a free nexhealth™ demo. Web dental clearance letter re _____ dob_____ mrn_____ to whom it may concern: Web request for medical clearance request for medical clearance patient name dear the above name patient has indicated that you are his/her physician.
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Our mutual patient, as noted above, is scheduled for dental treatment at our office. Learn more about digitizing your dental intake forms with nexhealth™. Ad the dental intake forms system that integrates with your pms. Just customize the form to match your dental office’s look. Web the american dental association (ada) offers a comprehensive health history form, for adults or.
FREE 44+ Medical Forms in PDF
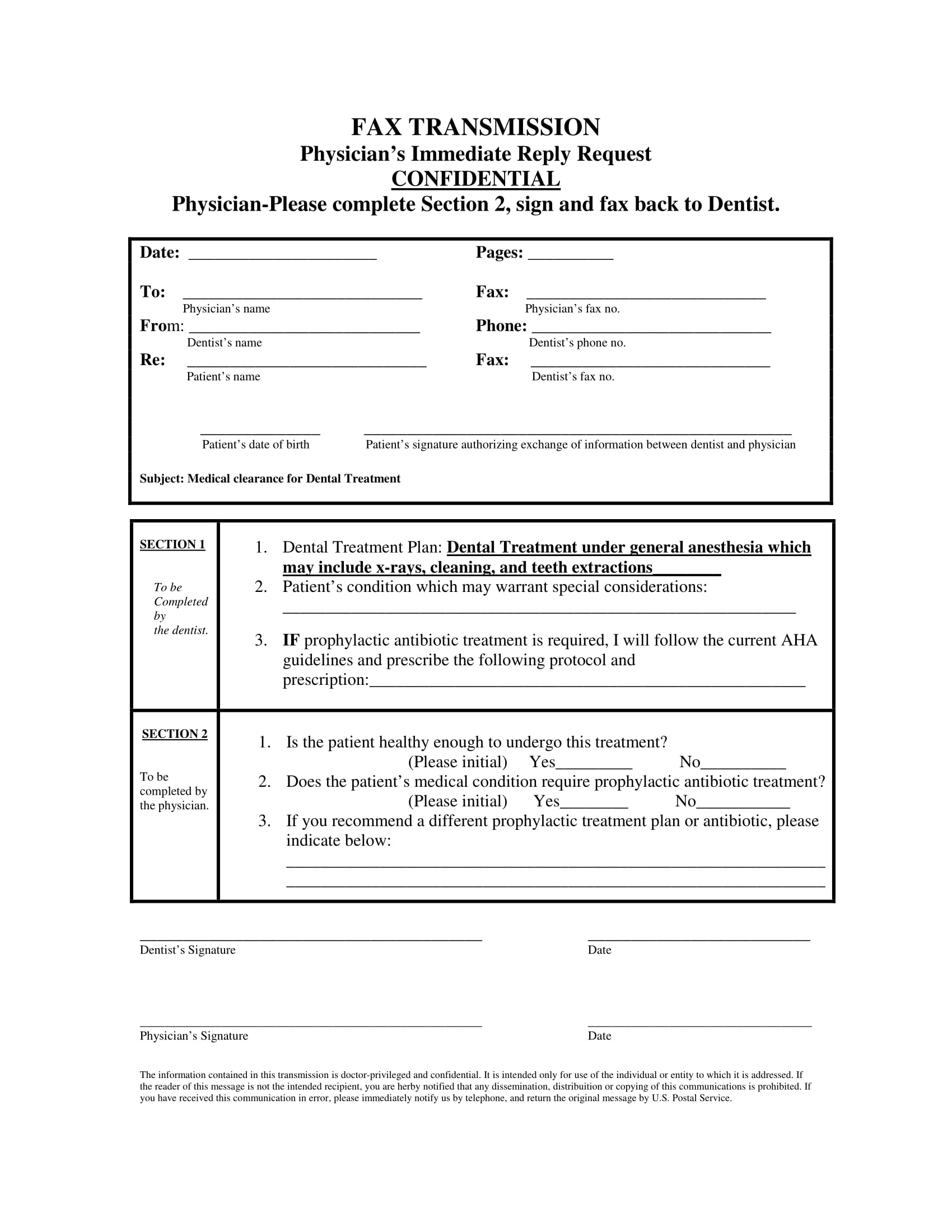
Save or instantly send your. Web medical clearance for dental treatment. Web medical clearance for dental treatment date: Web request for medical clearance request for medical clearance patient name dear the above name patient has indicated that you are his/her physician. Web this article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental.
Web Medical Clearance For Dental Treatment Date:
Easily fill out pdf blank, edit, and sign them. Web the cost for tooth extraction varies widely depending on whether the tooth is impacted. Try a free nexhealth™ demo. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental.
Save Or Instantly Send Your.
Huntington beach, ca 92646 o. Web medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical. Simple extraction usually costs between $75 and $200 per tooth, and may be more. Our mutual patient, as noted above, is scheduled for dental treatment at our office.
Web Are You Thinking About Getting Medical Clearance Form For Dental To Fill?
Our mutual patient noted above is scheduled to undergo total joint replacement surgery. Learn more about digitizing your dental intake forms with nexhealth™. Online with us legal forms. Web the physician will assess the risk of dental surgery based on the patient past and current condition in four categories:
Just Customize The Form To Match Your Dental Office’s Look.
Web the forms in this library are intended to be adapted for the organization's specific needs. Web dental clearance letter re _____ dob_____ mrn_____ to whom it may concern: Web medical clearance form (219)663 advanced dental concepts 10780 randolph street crown point, in 46307. Web this article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental procedures, such as cleanings,.