Patient Photo Release Form
Patient Photo Release Form - Web photo consent and release form patient name: Use get form or simply click on the template preview to open it in the editor. By signing this form, the patient affirms in understanding that the the images may be used for different purposes indicated hereunder. Upon expiration of this authorization, this hospital will not permit further release of any photograph, Web free patient photo release form for use with your photo clients. Save or instantly send your ready documents. Use the cross or check marks in the top toolbar to select your answers in the list boxes. _____ i consent for photographs and/or video images to be taken of me by aesthetispa, inc. I understand the images will be a part of my medical record and may be used for purposes of medical teaching or training or for marketing purposes (website, print, digital or. By consenting to the release of images, you agree that you.
_____ i consent for photographs and/or video images to be taken of me by aesthetispa, inc. Use get form or simply click on the template preview to open it in the editor. Upon expiration of this authorization, this hospital will not permit further release of any photograph, I understand the images will be a part of my medical record and may be used for purposes of medical teaching or training or for marketing purposes (website, print, digital or. Web complete patient photo release form online with us legal forms. Save or instantly send your ready documents. Web photo consent and release form patient name: By consenting to the release of images, you agree that you. Easily fill out pdf blank, edit, and sign them. By signing this form, the patient affirms in understanding that the the images may be used for different purposes indicated hereunder.
Save or instantly send your ready documents. Use the cross or check marks in the top toolbar to select your answers in the list boxes. Web complete patient photo release form online with us legal forms. Web free patient photo release form for use with your photo clients. By signing this form, the patient affirms in understanding that the the images may be used for different purposes indicated hereunder. Start completing the fillable fields and carefully type in required information. I understand the images will be a part of my medical record and may be used for purposes of medical teaching or training or for marketing purposes (website, print, digital or. Web photo consent and release form patient name: Use get form or simply click on the template preview to open it in the editor. Go paperless and immediately store your consent to your records.
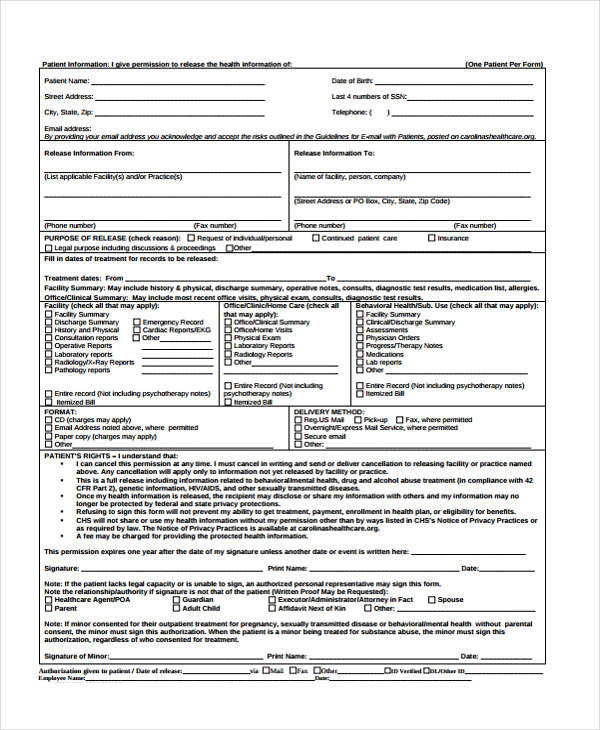
FREE 12+ Sample Medical Records Release Forms in PDF MS Word Excel
Use get form or simply click on the template preview to open it in the editor. Web a patient photo release form is a legal document that grants healthcare providers or medical institutions the permission to use photographs or images of a patient for specific purposes related to their medical care. Web photo consent and release form patient name: Go.
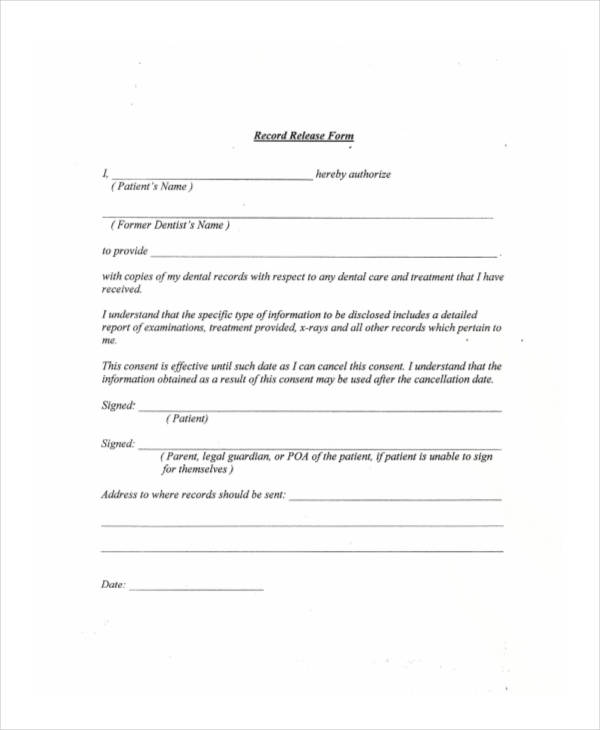
FREE 19+ Patient Release Forms in PDF MS Word
Web patient photo release form. Web use this patient photo release form template and get your photo release consent from patients immediately! Remove any clauses you don't need, update the cover page and send out for signing online. _____ i consent for photographs and/or video images to be taken of me by aesthetispa, inc. Use the cross or check marks.
FREE 19+ Patient Release Forms in PDF MS Word
Upon expiration of this authorization, this hospital will not permit further release of any photograph, By signing this form, the patient affirms in understanding that the the images may be used for different purposes indicated hereunder. Start completing the fillable fields and carefully type in required information. Web a patient photo release form is a legal document that grants healthcare.
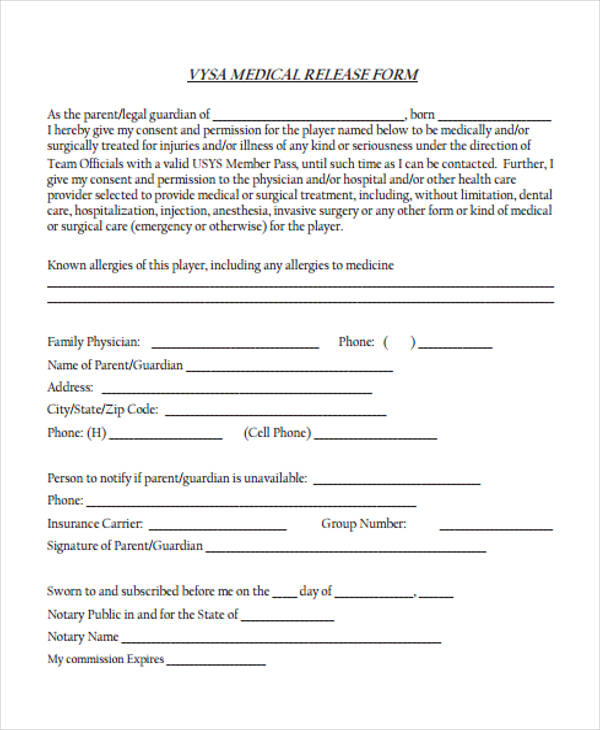
FREE 19+ Patient Release Forms in PDF MS Word
Start completing the fillable fields and carefully type in required information. Go paperless and immediately store your consent to your records. Upon expiration of this authorization, this hospital will not permit further release of any photograph, Web patient photo release form. This form seeks for the consent for photographs to be taken by the medical institution through a doctor or.
FREE 21+ Sample Patient Release Forms in PDF MS Word
By consenting to the release of images, you agree that you. Web use this patient photo release form template and get your photo release consent from patients immediately! Start completing the fillable fields and carefully type in required information. Use the cross or check marks in the top toolbar to select your answers in the list boxes. Use get form.

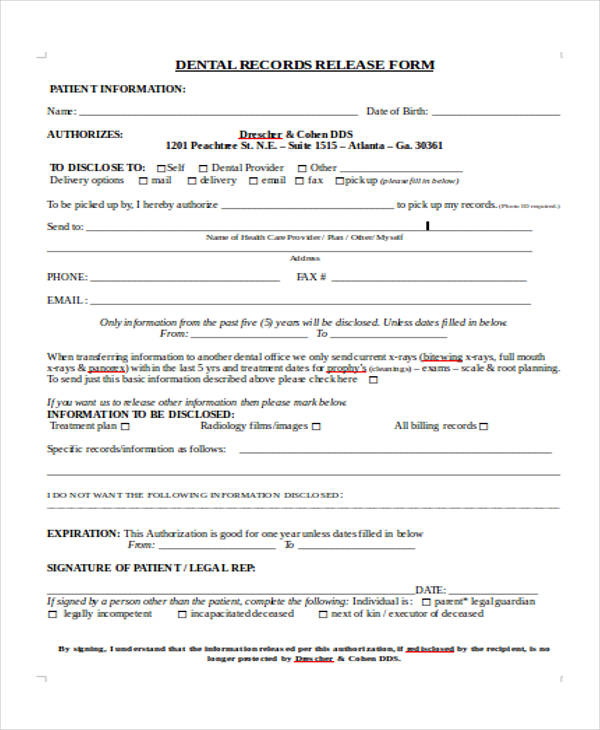
FREE 31+ Medical Release Forms in PDF
Save or instantly send your ready documents. Start completing the fillable fields and carefully type in required information. Web photo consent and release form patient name: Remove any clauses you don't need, update the cover page and send out for signing online. Use the cross or check marks in the top toolbar to select your answers in the list boxes.
FREE 19+ Patient Release Forms in PDF MS Word
Remove any clauses you don't need, update the cover page and send out for signing online. Save or instantly send your ready documents. Web photo consent and release form patient name: This form seeks for the consent for photographs to be taken by the medical institution through a doctor or a representative. Use the cross or check marks in the.
FREE 23+ Patient Release Forms in PDF MS Word
By consenting to the release of images, you agree that you. This form seeks for the consent for photographs to be taken by the medical institution through a doctor or a representative. Easily fill out pdf blank, edit, and sign them. Web use this patient photo release form template and get your photo release consent from patients immediately! Use the.
FREE 21+ Sample Patient Release Forms in PDF MS Word
Easily fill out pdf blank, edit, and sign them. Use get form or simply click on the template preview to open it in the editor. Web photo consent and release form patient name: Upon expiration of this authorization, this hospital will not permit further release of any photograph, Start completing the fillable fields and carefully type in required information.
FREE 9+ Sample Medical Records Release Forms in PDF MS Word
Web photo consent and release form patient name: Web complete patient photo release form online with us legal forms. By signing this form, the patient affirms in understanding that the the images may be used for different purposes indicated hereunder. Easily fill out pdf blank, edit, and sign them. Web a patient photo release form is a legal document that.
Go Paperless And Immediately Store Your Consent To Your Records.
By signing this form, the patient affirms in understanding that the the images may be used for different purposes indicated hereunder. Web photo consent and release form patient name: Web patient photo release form. Web use this patient photo release form template and get your photo release consent from patients immediately!
Web Free Patient Photo Release Form For Use With Your Photo Clients.
Web complete patient photo release form online with us legal forms. Use get form or simply click on the template preview to open it in the editor. Web a patient photo release form is a legal document that grants healthcare providers or medical institutions the permission to use photographs or images of a patient for specific purposes related to their medical care. Start completing the fillable fields and carefully type in required information.
By Consenting To The Release Of Images, You Agree That You.
This form seeks for the consent for photographs to be taken by the medical institution through a doctor or a representative. _____ i consent for photographs and/or video images to be taken of me by aesthetispa, inc. Save or instantly send your ready documents. Remove any clauses you don't need, update the cover page and send out for signing online.
Upon Expiration Of This Authorization, This Hospital Will Not Permit Further Release Of Any Photograph,
Use the cross or check marks in the top toolbar to select your answers in the list boxes. Easily fill out pdf blank, edit, and sign them. I understand the images will be a part of my medical record and may be used for purposes of medical teaching or training or for marketing purposes (website, print, digital or.