Medical Accommodations Request Form 2022-23
Medical Accommodations Request Form 2022-23 - Web if the request is for a diagnosis of allergies/anaphylaxis, diabetes, or seizure disorder, please complete the medical accommodations request form addendum. Web how to request health services educational and other accommodations paraprofessionals transportation accommodations frequently asked questions parent communications medically necessary instruction summary section 504 of the rehabilitation act of 1973 requires public schools to offer accommodations for eligible. Date of medical documentation request: Submit the completed medical accommodations request form to your school’s 504 coordinator, along with Part i—requester’s contact information requester’s name: Easily fill out pdf blank, edit, and sign them. Download adobe reader ™ print page email page last reviewed: Americans with disabilities citizens and consumers. Save or instantly send your ready documents. Please attach additional documentation, if needed student name:
☐ acute ☐ chronic expected duration of accommodation: Americans with disabilities citizens and consumers. Download adobe reader ™ print page email page last reviewed: Hrm 2300.1 pdf versions of forms use adobe reader ™. Web how to request health services educational and other accommodations paraprofessionals transportation accommodations frequently asked questions parent communications medically necessary instruction summary section 504 of the rehabilitation act of 1973 requires public schools to offer accommodations for eligible. Web if the request is for a diagnosis of allergies/anaphylaxis, diabetes, or seizure disorder, please complete the medical accommodations request form addendum. Easily fill out pdf blank, edit, and sign them. Please return this form to the employee or directly to the agency within 15 days of receipt. Please attach additional documentation, if needed student name: Part i—requester’s contact information requester’s name:
Please attach additional documentation, if needed student name: Download adobe reader ™ print page email page last reviewed: Part i—requester’s contact information requester’s name: Save or instantly send your ready documents. Easily fill out pdf blank, edit, and sign them. Web if the request is for a diagnosis of allergies/anaphylaxis, diabetes, or seizure disorder, please complete the medical accommodations request form addendum. ☐ acute ☐ chronic expected duration of accommodation: Request for reasonable accommodation form #: Please return this form to the employee or directly to the agency within 15 days of receipt. Americans with disabilities citizens and consumers.

Reasonable Request Form Housing certify letter
Request for reasonable accommodation form #: Please attach additional documentation, if needed student name: Web if the request is for a diagnosis of allergies/anaphylaxis, diabetes, or seizure disorder, please complete the medical accommodations request form addendum. Part i—requester’s contact information requester’s name: Americans with disabilities citizens and consumers.

AL MVT 57 2012 Fill and Sign Printable Template Online US Legal Forms
Submit the completed medical accommodations request form to your school’s 504 coordinator, along with Request for reasonable accommodation form #: Hrm 2300.1 pdf versions of forms use adobe reader ™. Americans with disabilities citizens and consumers. Please attach additional documentation, if needed student name:
Web how to request health services educational and other accommodations paraprofessionals transportation accommodations frequently asked questions parent communications medically necessary instruction summary section 504 of the rehabilitation act of 1973 requires public schools to offer accommodations for eligible. Easily fill out pdf blank, edit, and sign them. Save or instantly send your ready documents. Request for reasonable accommodation form #:.

TAMU Medical Questionnaire For Reasonable Requests 2020
Save or instantly send your ready documents. Easily fill out pdf blank, edit, and sign them. Part i—requester’s contact information requester’s name: Americans with disabilities citizens and consumers. Please attach additional documentation, if needed student name:
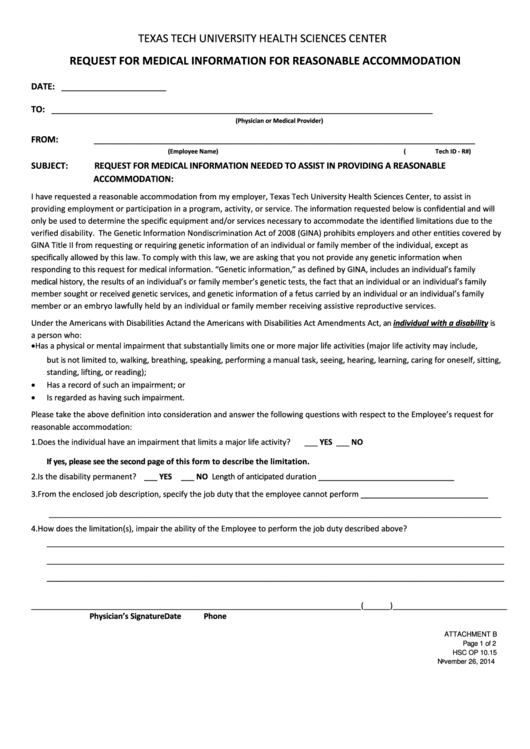
Request For Medical Information For Reasonable Form
Request for reasonable accommodation form #: Date of medical documentation request: Please attach additional documentation, if needed student name: Easily fill out pdf blank, edit, and sign them. Americans with disabilities citizens and consumers.

MEDICAL INQUIRY FORM IN RESPONSE TO AN REQUEST
Submit the completed medical accommodations request form to your school’s 504 coordinator, along with Please attach additional documentation, if needed student name: Download adobe reader ™ print page email page last reviewed: ☐ acute ☐ chronic expected duration of accommodation: Web how to request health services educational and other accommodations paraprofessionals transportation accommodations frequently asked questions parent communications medically necessary.

Home StandishSterling Central High School
Hrm 2300.1 pdf versions of forms use adobe reader ™. Date of medical documentation request: Easily fill out pdf blank, edit, and sign them. Save or instantly send your ready documents. Web if the request is for a diagnosis of allergies/anaphylaxis, diabetes, or seizure disorder, please complete the medical accommodations request form addendum.
reasonable verification form
Please return this form to the employee or directly to the agency within 15 days of receipt. Hrm 2300.1 pdf versions of forms use adobe reader ™. Easily fill out pdf blank, edit, and sign them. Save or instantly send your ready documents. Please attach additional documentation, if needed student name:
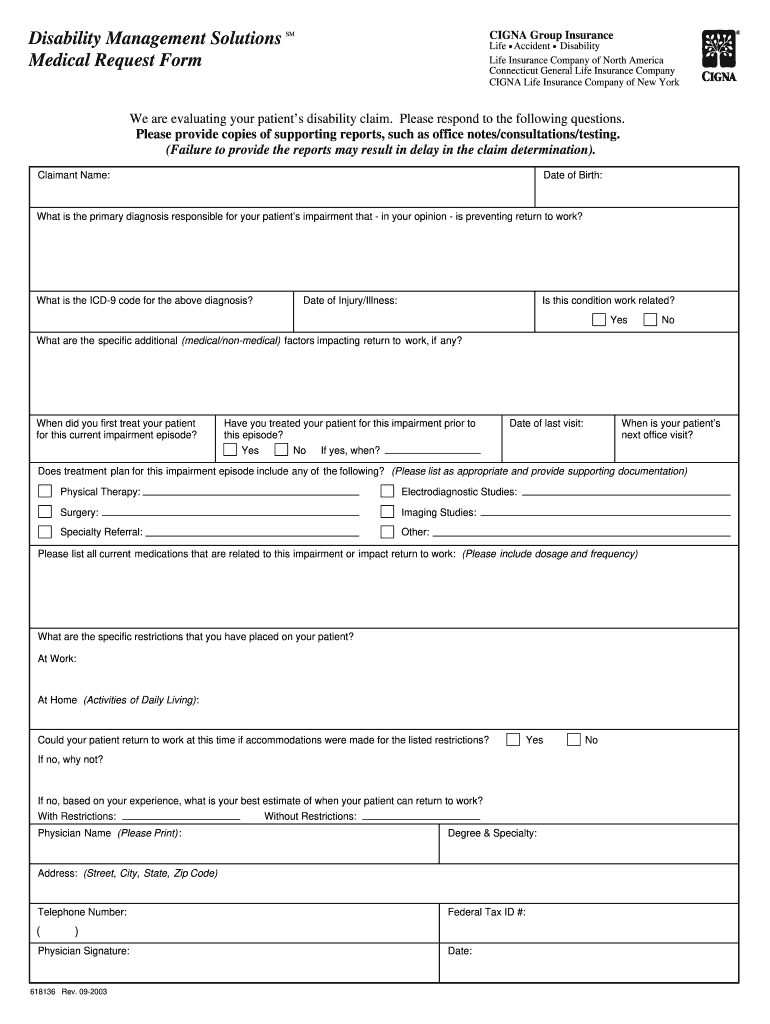
Cigna Ada Request Form Fill Out and Sign Printable PDF
Date of medical documentation request: Save or instantly send your ready documents. ☐ acute ☐ chronic expected duration of accommodation: Please return this form to the employee or directly to the agency within 15 days of receipt. Web how to request health services educational and other accommodations paraprofessionals transportation accommodations frequently asked questions parent communications medically necessary instruction summary section.
Form Cnp925 Medical Statement To Request Special Meals And Or
Submit the completed medical accommodations request form to your school’s 504 coordinator, along with Hrm 2300.1 pdf versions of forms use adobe reader ™. Please return this form to the employee or directly to the agency within 15 days of receipt. Web if the request is for a diagnosis of allergies/anaphylaxis, diabetes, or seizure disorder, please complete the medical accommodations.
Please Return This Form To The Employee Or Directly To The Agency Within 15 Days Of Receipt.
Web how to request health services educational and other accommodations paraprofessionals transportation accommodations frequently asked questions parent communications medically necessary instruction summary section 504 of the rehabilitation act of 1973 requires public schools to offer accommodations for eligible. Americans with disabilities citizens and consumers. Date of medical documentation request: Save or instantly send your ready documents.
Please Attach Additional Documentation, If Needed Student Name:
Easily fill out pdf blank, edit, and sign them. Submit the completed medical accommodations request form to your school’s 504 coordinator, along with Hrm 2300.1 pdf versions of forms use adobe reader ™. Web if the request is for a diagnosis of allergies/anaphylaxis, diabetes, or seizure disorder, please complete the medical accommodations request form addendum.
Part I—Requester’s Contact Information Requester’s Name:
☐ acute ☐ chronic expected duration of accommodation: Request for reasonable accommodation form #: Download adobe reader ™ print page email page last reviewed: